

Implant-based Breast Reconstruction after Mastectomy for Breast Cancer: A Systematic Review and Meta-analysis
- PMID: 35317462
- PMCID: PMC8932484
- DOI: 10.1097/GOX.0000000000004179
Implant-based Breast Reconstruction after Mastectomy for Breast Cancer: A Systematic Review and Meta-analysis
Abstract
Women undergoing implant-based reconstruction (IBR) after mastectomy for breast cancer have numerous options, including timing of IBR relative to radiation and chemotherapy, implant materials, anatomic planes, and use of human acellular dermal matrices. We conducted a systematic review to evaluate these options.
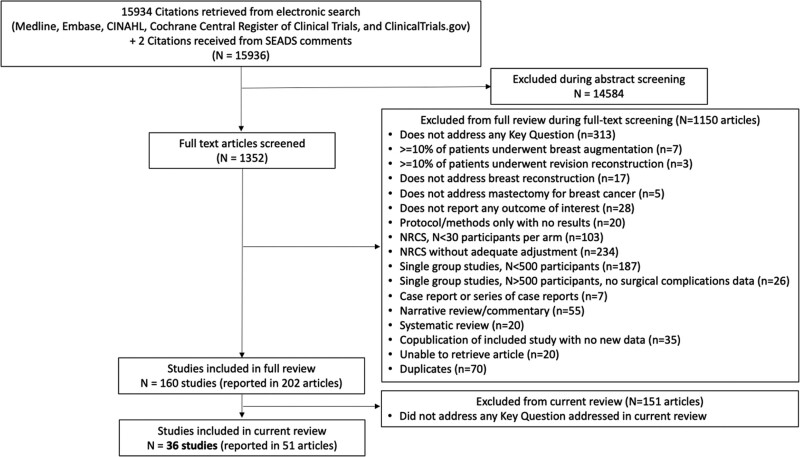
Methods: We searched Medline, Embase, Cochrane CENTRAL, CINAHL, and ClinicalTrials.gov for studies, from inception to March 23, 2021, without language restriction. We assessed risk of bias and strength of evidence (SoE) using standard methods.
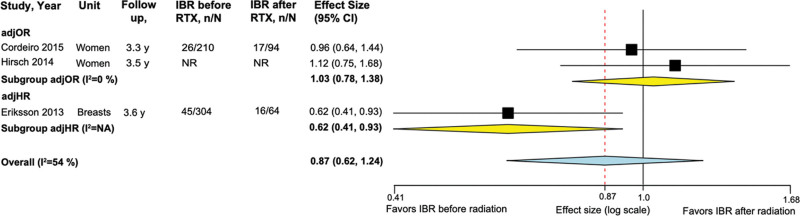
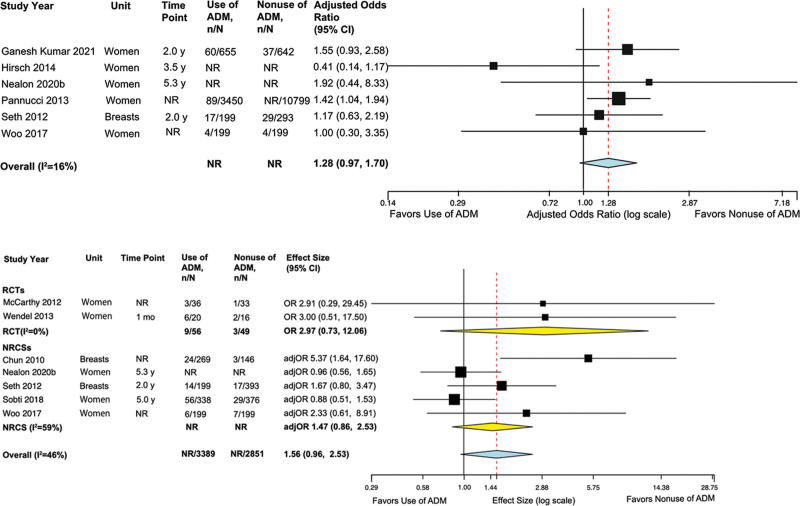
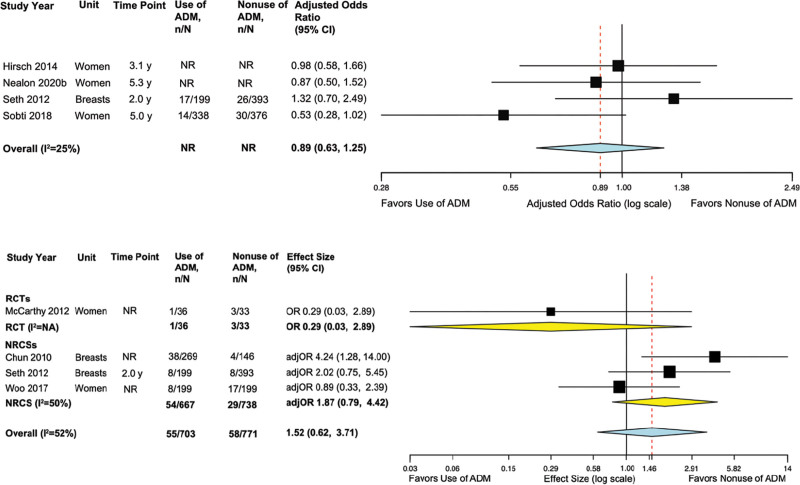
Results: We screened 15,936 citations. Thirty-six mostly high or moderate risk of bias studies (48,419 patients) met criteria. Timing of IBR before or after radiation may result in comparable physical, psychosocial, and sexual well-being, and satisfaction with breasts (all low SoE), and probably comparable risks of implant failure/loss or explantation (moderate SoE). No studies addressed timing relative to chemotherapy. Silicone and saline implants may result in clinically comparable satisfaction with breasts (low SoE). Whether the implant is in the prepectoral or total submuscular plane may not impact risk of infections (low SoE). Acellular dermal matrix use probably increases the risk of implant failure/loss or need for explant surgery (moderate SoE) and may increase the risk of infections (low SoE). Risks of seroma and unplanned repeat surgeries for revision are probably comparable (moderate SoE), and risk of necrosis may be comparable with or without human acellular dermal matrices (low SoE).
Conclusions: Evidence regarding IBR options is mostly of low SoE. New high-quality research is needed, especially for timing, implant materials, and anatomic planes of implant placement.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Figures
References
-
- American Society of Plastic Surgeons. 2019 plastic surgery statistics report. Available at https://www.plasticsurgery.org/documents/News/Statistics/2019/plastic-su.... Accessed February 13, 2021.
-
- Saldanha IJ, Cao W, Broyles JM, et al. . Breast Reconstruction after Mastectomy: A Systematic Review and Meta-Analysis. Comparative Effectiveness Review No. 245. Rockville, Md.: Agency for Healthcare Research and Quality; 2021. Available at 10.23970/AHRQEPCCER245. Accessed July 16, 2021. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous