

Gene Therapy With the N-Terminus of Junctophilin-2 Improves Heart Failure in Mice
- PMID: 35317607
- PMCID: PMC9050933
- DOI: 10.1161/CIRCRESAHA.121.320680
Gene Therapy With the N-Terminus of Junctophilin-2 Improves Heart Failure in Mice
Abstract
Background: Transcriptional remodeling is known to contribute to heart failure (HF). Targeting stress-dependent gene expression mechanisms may represent a clinically relevant gene therapy option. We recently uncovered a salutary mechanism in the heart whereby JP2 (junctophilin-2), an essential component of the excitation-contraction coupling apparatus, is site-specifically cleaved and releases an N-terminal fragment (JP2NT [N-terminal fragment of JP2]) that translocates into the nucleus and functions as a transcriptional repressor of HF-related genes. This study aims to determine whether JP2NT can be leveraged by gene therapy techniques for attenuating HF progression in a preclinical pressure overload model.
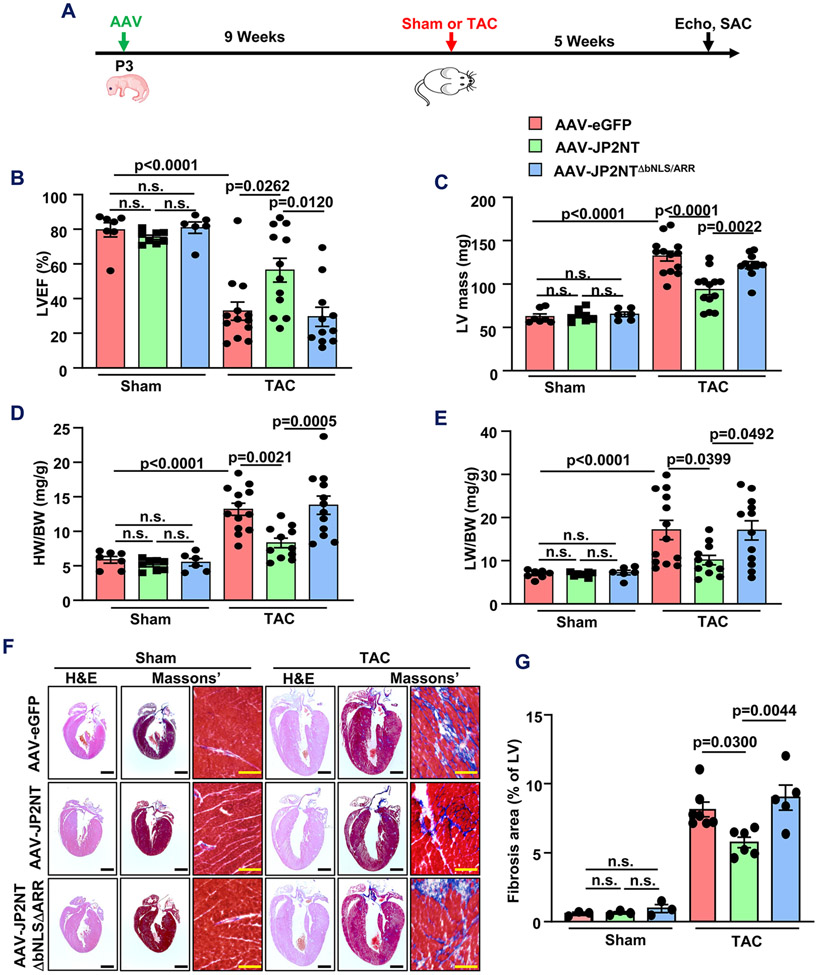
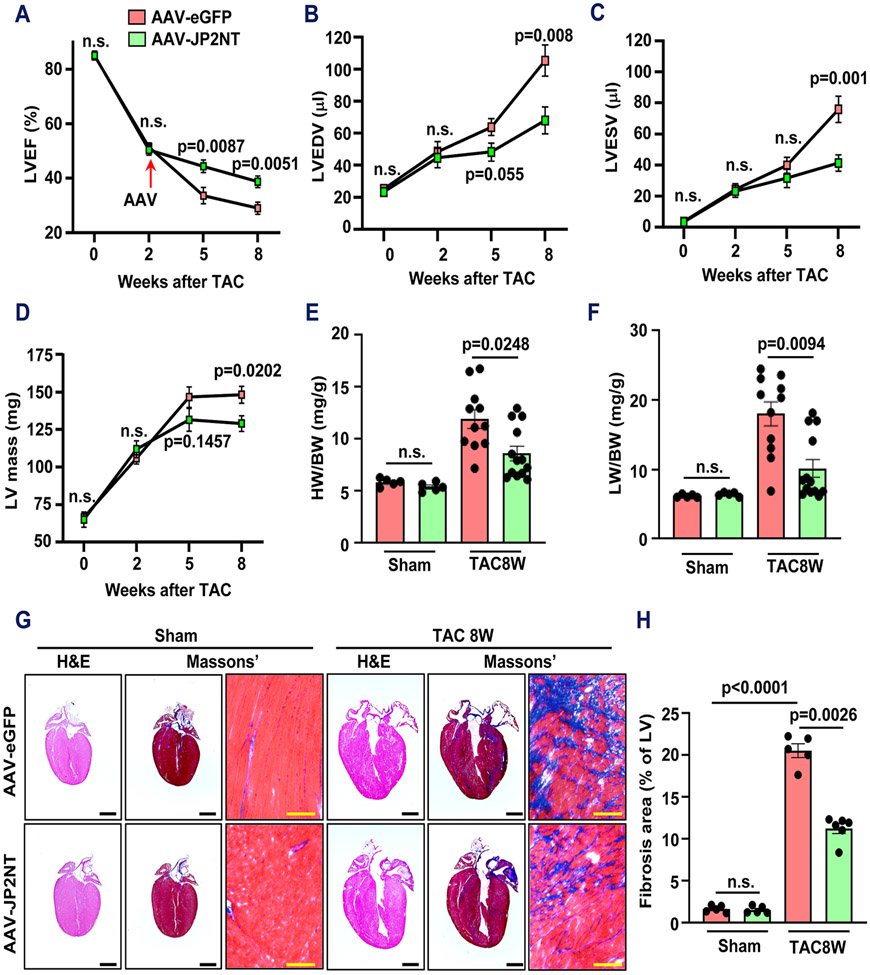
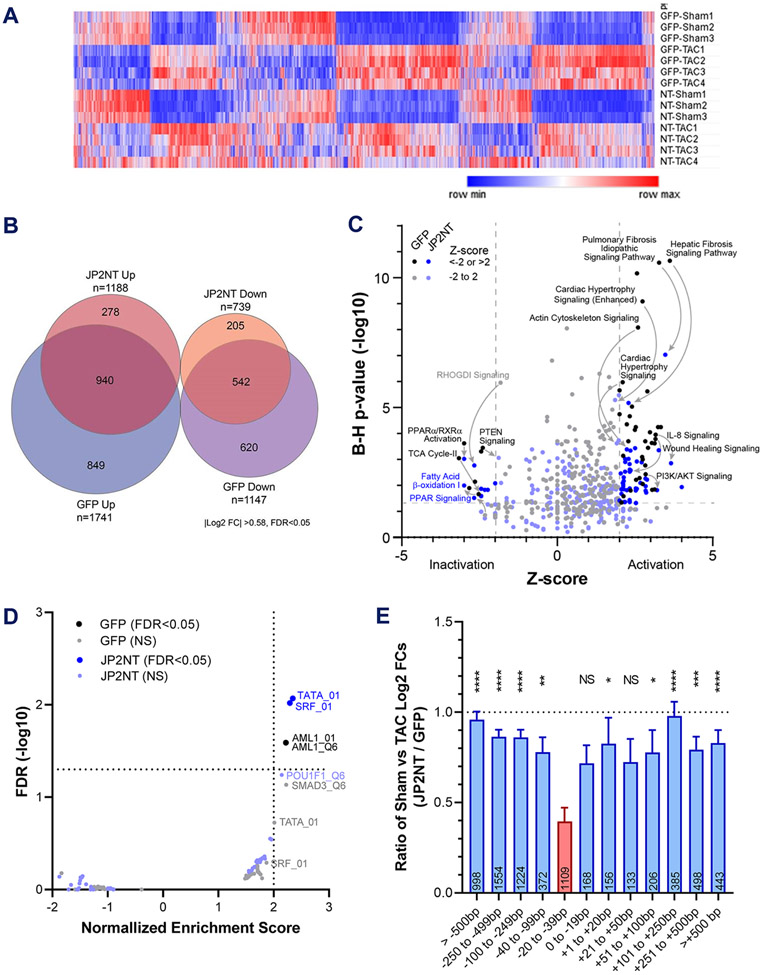
Methods: We intraventricularly injected adeno-associated virus (AAV) (2/9) vectors expressing eGFP (enhanced green fluorescent protein), JP2NT, or DNA-binding deficient JP2NT (JP2NTΔbNLS/ARR) into neonatal mice and induced cardiac stress by transaortic constriction (TAC) 9 weeks later. We also treated mice with established moderate HF from TAC stress with either AAV-JP2NT or AAV-eGFP. RNA-sequencing analysis was used to reveal changes in hypertrophic and HF-related gene transcription by JP2NT gene therapy after TAC. Echocardiography, confocal imaging, and histology were performed to evaluate heart function and pathological myocardial remodeling following stress.
Results: Mice preinjected with AAV-JP2NT exhibited ameliorated cardiac remodeling following TAC. The JP2NT DNA-binding domain is required for cardioprotection as its deletion within the AAV-JP2NT vector prevented improvement in TAC-induced cardiac dysfunction. Functional and histological data suggest that JP2NT gene therapy after the onset of cardiac dysfunction is effective at slowing the progression of HF. RNA-sequencing analysis further revealed a broad reversal of hypertrophic and HF-related gene transcription by JP2NT overexpression after TAC.
Conclusions: Our prevention- and intervention-based approaches here demonstrated that AAV-mediated delivery of JP2NT into the myocardium can attenuate stress-induced transcriptional remodeling and the development of HF when administered either before or after cardiac stress initiation. Our data indicate that JP2NT gene therapy holds great potential as a novel therapeutic for treating hypertrophy and HF.
Keywords: genetic therapy; heart failure; hypertrophy; junctophilin.
Figures



Comment in
-
Junctophillin-2: Coupling Hopes for Cardiac Gene Therapy to Gene Transcription.Circ Res. 2022 Apr 29;130(9):1318-1320. doi: 10.1161/CIRCRESAHA.122.321066. Epub 2022 Apr 28. Circ Res. 2022. PMID: 35482830 No abstract available.
References
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, Elkind MSV, Evenson KR, Ferguson JF, Gupta DK, Khan SS, Kissela BM, Knutson KL, Lee CD, Lewis TT, Liu J, Loop MS, Lutsey PL, Ma J, Mackey J, Martin SS, Matchar DB, Mussolino ME, Navaneethan SD, Perak AM, Roth GA, Samad Z, Satou GM, Schroeder EB, Shah SH, Shay CM, Stokes A, VanWagner LB, Wang NY, Tsao CW, American Heart Association Council on E, Prevention Statistics C and Stroke Statistics S. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation. 2021;143:e254–e743. - PubMed
-
- Lohse MJ, Engelhardt S and Eschenhagen T. What is the role of beta-adrenergic signaling in heart failure? Circulation research. 2003;93:896–906. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
