

Esophageal tuberculosis induced dysphagia: a case report
- PMID: 35317747
- PMCID: PMC8939207
- DOI: 10.1186/s12876-022-02211-2
Esophageal tuberculosis induced dysphagia: a case report
Abstract
Background: Patients can present for a wide variety of etiologies for dysphagia, and it is important to consider less common causes once common etiologies have been ruled out. Extrapulmonary Mycobacterium tuberculosis (TB) presentations are rare to see in the western populations due to relative lack of TB exposure and overall less immunocompromised populations, but should be considered for at-risk patients. Gastrointestinal (GI) TB is rare, and the GI tract is considered only the sixth most frequent site of extrapulmonary TB (EPTB).
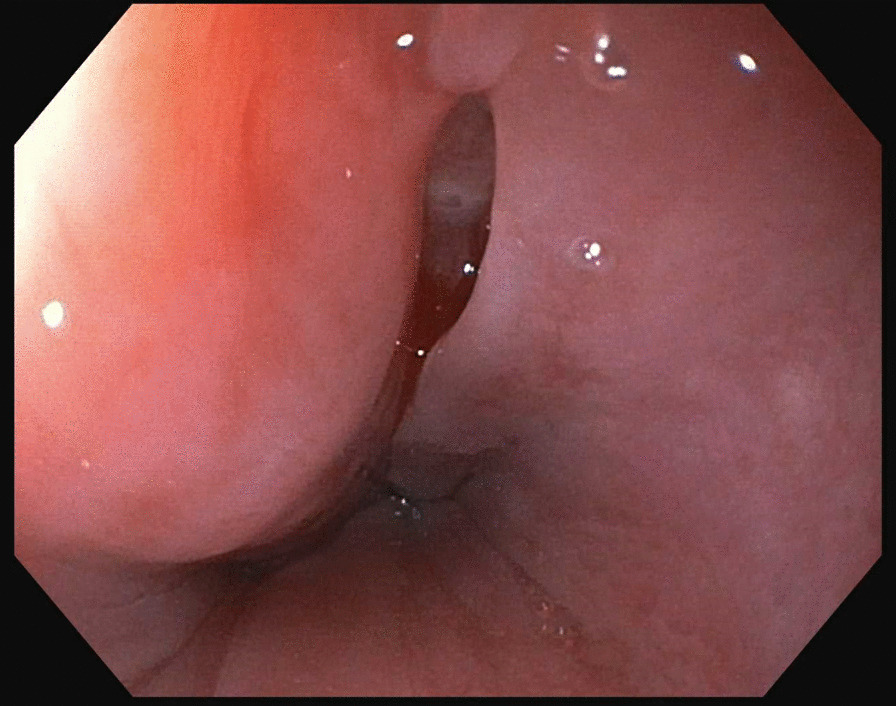
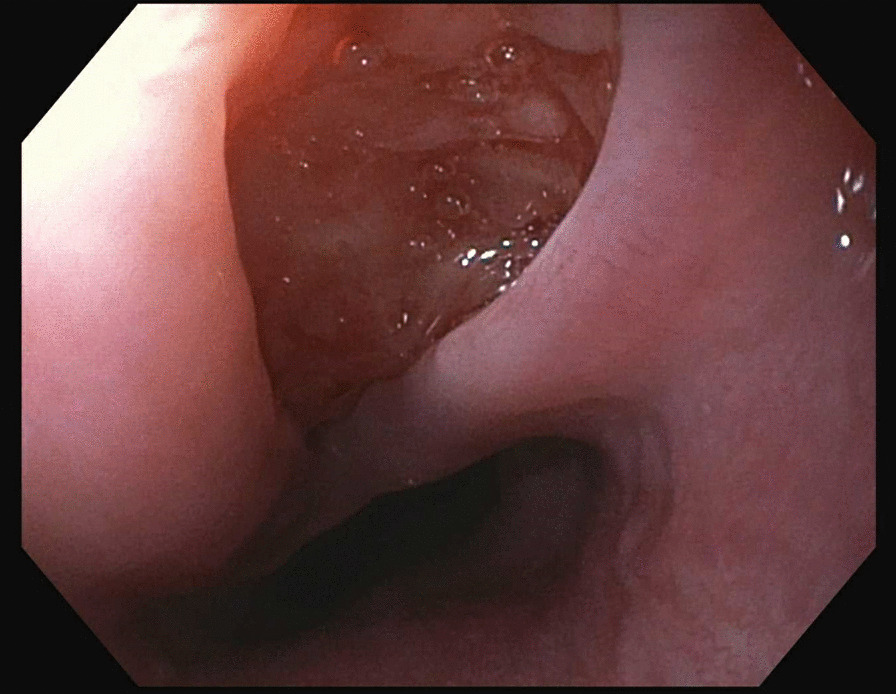
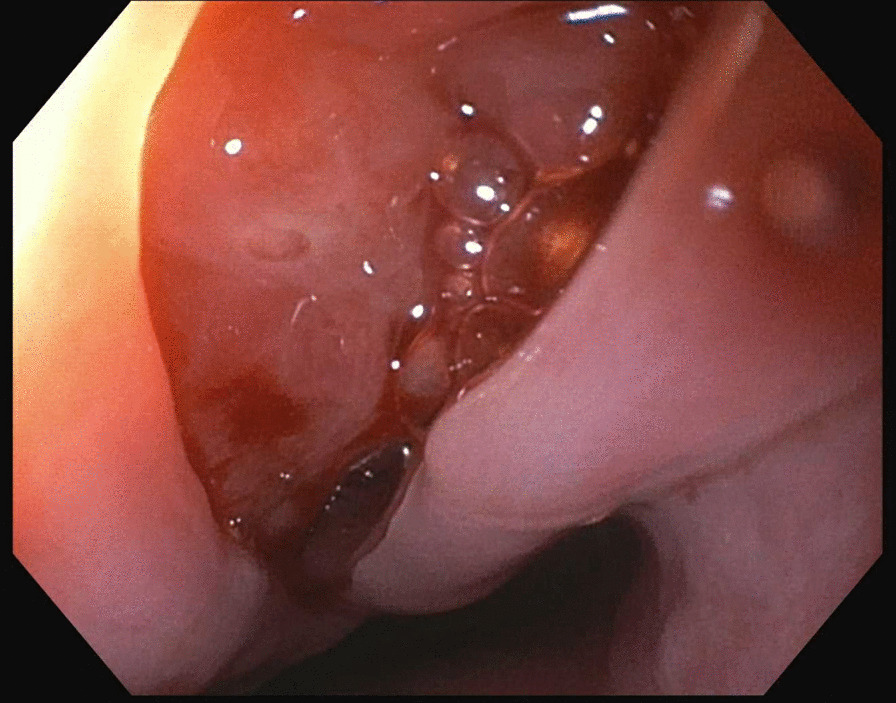
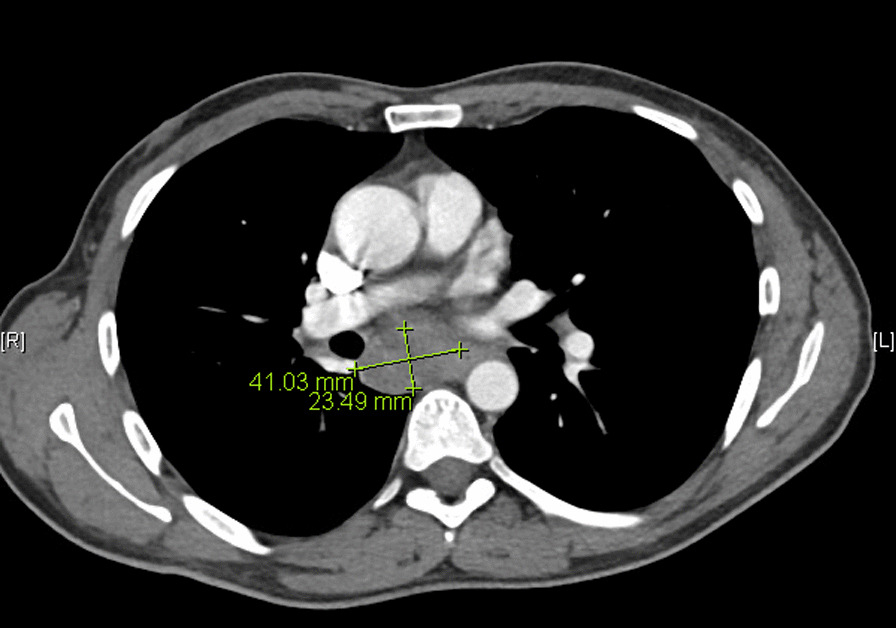
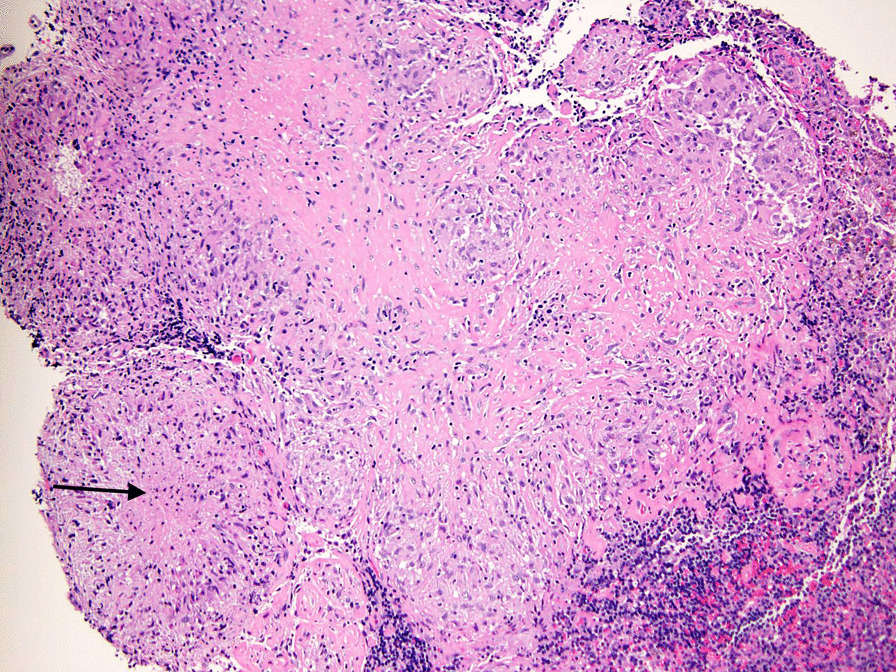
Case presentation: This is a case report of a 35-year-old Ethiopian male presenting with dysphagia and retrosternal odynophagia who was found to have infiltration of mediastinal lymphadenopathy into the esophageal wall secondary to TB. This patient underwent an upper endoscopy, which revealed a linear 2 cm full thickness mucosal defect in the middle esophagus concerning for an infiltrative process with full thickness tear. Computed tomography (CT) of the chest demonstrated a subcarinal soft tissue mass that was inseparable from the esophagus. He was referred to thoracic surgery and underwent an exploratory mediastinal dissection. A mediastinoscopy scope was inserted and the mediastinal dissection was made until the subcarinal nodes were identified and removed. Biopsy results showed necrotizing and non-necrotizing granulomas, and acid-fast bacilli (AFB) culture from the surgically removed lymph node showed Mycobacterium TB complex growth. He had no known TB exposures and did not have any TB risk factors. He then followed up in infectious disease clinic and was managed with anti-tuberculosis treatment (ATT) with complete resolution of symptoms.
Conclusions: Our patient was ultimately found to have esophageal TB secondary to mediastinal invasion into the esophageal wall from lymphadenopathy associated with TB. This is an extremely rare presentation in western populations due to diminished exposure rates and overall less immunocompromised populations compared to impoverished countries with increased TB exposure and human immunodeficiency virus (HIV) infection rates. Although TB is not as commonly seen in western populations, it should be considered on the differential for any atypical presentations of GI diseases for patients with clinical or geographic risk factors.
Keywords: Esophageal tuberculosis; Esophageal tuberculosis induced dysphagia; Mycobacterium tuberculosis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rathi P, Gambhire P. Abdominal tuberculosis. J Assoc Physicians India. 2016;64(2):38–47. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
