

Variation in statin prescription among veterans with HIV and known atherosclerotic cardiovascular disease
- PMID: 35318028
- PMCID: PMC9976623
- DOI: 10.1016/j.ahj.2022.03.006
Variation in statin prescription among veterans with HIV and known atherosclerotic cardiovascular disease
Abstract
Background: People with HIV have increased atherosclerotic cardiovascular disease (ASCVD) risk, worse outcomes following incident ASCVD, and experience gaps in cardiovascular care, highlighting the need to improve delivery of preventive therapies in this population.
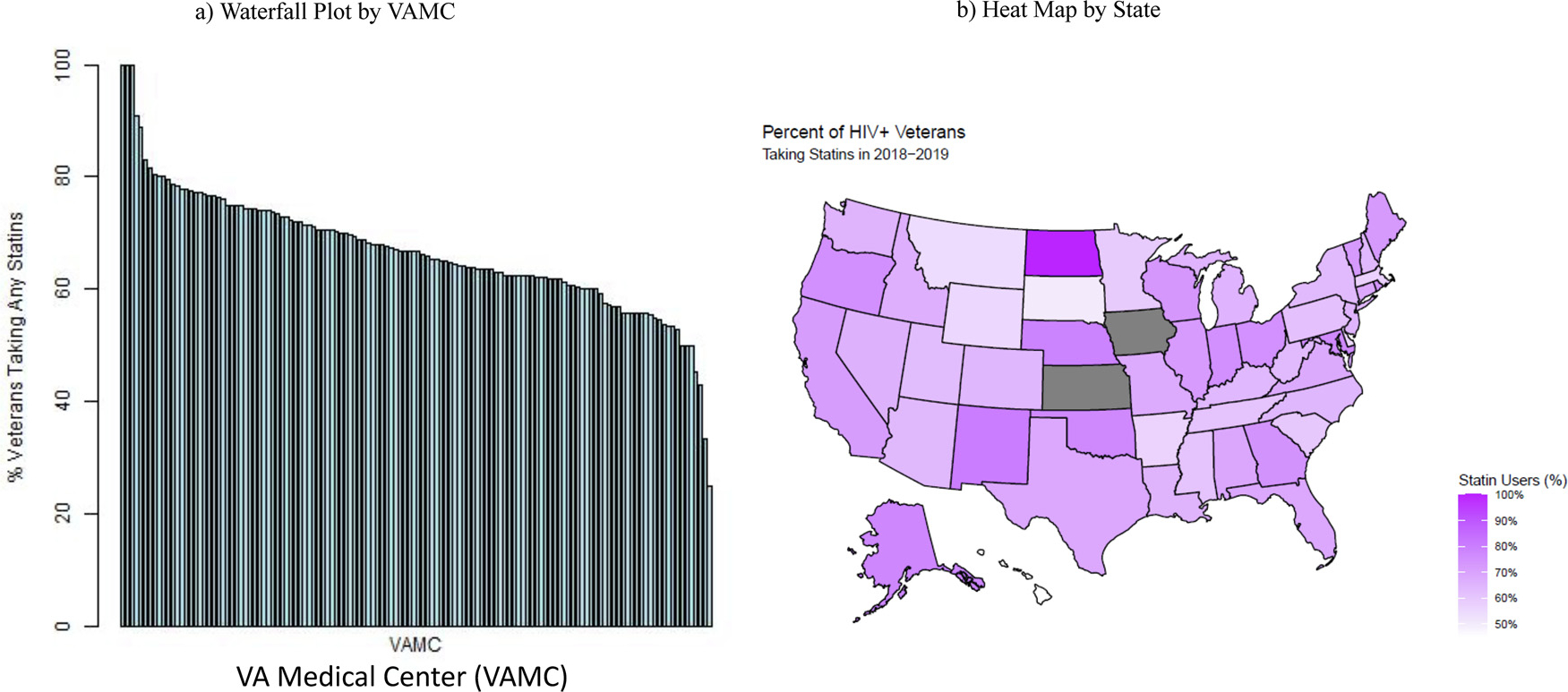
Objective: Assess patient-level correlates and inter-facility variations in statin prescription among Veterans with HIV and known ASCVD.
Methods: We studied Veterans with HIV and existing ASCVD, ie, coronary artery disease (CAD), ischemic cerebrovascular disease (ICVD), and peripheral arterial disease (PAD), who received care across 130 VA medical centers for the years 2018-2019. We assessed correlates of statin prescription using two-level hierarchical multivariable logistic regression. Median odds ratios (MORs) were used to quantify inter-facility variation in statin prescription.
Results: Nine thousand six hundred eight Veterans with HIV and known ASCVD (mean age 64.3 ± 8.9 years, 97% male, 48% Black) were included. Only 68% of the participants were prescribed any-statin. Substantially higher statin prescription was observed for those with diabetes (adjusted odds ratio [OR] = 2.3, 95% confidence interval [CI], 2.0-2.6), history of coronary revascularization (OR = 4.0, CI, 3.2-5.0), and receiving antiretroviral therapy (OR = 3.0, CI, 2.7-3.4). Blacks (OR = 0.7, CI, 0.6-0.9), those with non-coronary ASCVD, ie, ICVD and/or PAD only, (OR 0.53, 95% CI: 0.48-0.57), and those with history of illicit substance use (OR=0.7, CI, 0.6-0.9) were less likely to be prescribed statins. There was significant variation in statin prescription across VA facilities (10th, 90th centile: 55%, 78%), with an estimated 20% higher likelihood of difference in statin prescription practice for two clinically similar individuals treated at two comparable facilities (adjusted MOR = 1.21, CI, 1.18-1.24), and a greater variation observed for Blacks or those with non-coronary ASCVD or history of illicit drug use.
Conclusion: In an analysis of large-scale VA data, we found suboptimal statin prescription and significant interfacility variation in statin prescription among Veterans with HIV and known ASCVD, particularly among Blacks and those with a history of non-coronary ASCVD.
Keywords: CVD; Cardiovascular disease; HIV; Health care quality; Health services; Human immunodeficiency virus; Statin.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Statin prescription rates and their facility-level variation in patients with peripheral artery disease and ischemic cerebrovascular disease: Insights from the Department of Veterans Affairs.Vasc Med. 2018 Jun;23(3):232-240. doi: 10.1177/1358863X18758914. Epub 2018 Mar 30. Vasc Med. 2018. PMID: 29600737
-
Significant Facility-Level Variation in Utilization of and Adherence with Secondary Prevention Therapies Among Patients with Premature Atherosclerotic Cardiovascular Disease: Insights from the VITAL (Veterans wIth premaTure AtheroscLerosis) Registry7.Cardiovasc Drugs Ther. 2022 Feb;36(1):93-102. doi: 10.1007/s10557-020-07125-3. Epub 2021 Jan 5. Cardiovasc Drugs Ther. 2022. PMID: 33400053
-
Sex-Related Disparities in Cardiovascular Health Care Among Patients With Premature Atherosclerotic Cardiovascular Disease.JAMA Cardiol. 2021 Jul 1;6(7):782-790. doi: 10.1001/jamacardio.2021.0683. JAMA Cardiol. 2021. PMID: 33881448 Free PMC article.
-
Nonobstructive Coronary Artery Disease by Coronary CT Angiography Improves Risk Stratification and Allocation of Statin Therapy.JACC Cardiovasc Imaging. 2017 Sep;10(9):1031-1038. doi: 10.1016/j.jcmg.2016.10.022. Epub 2017 Mar 15. JACC Cardiovasc Imaging. 2017. PMID: 28330658 Free PMC article. Review.
-
2017 Taiwan lipid guidelines for high risk patients.J Formos Med Assoc. 2017 Apr;116(4):217-248. doi: 10.1016/j.jfma.2016.11.013. Epub 2017 Feb 24. J Formos Med Assoc. 2017. PMID: 28242176 Review.
Cited by
-
Nurse-Led Strategy to Improve Blood Pressure and Cholesterol Level Among People With HIV: A Randomized Clinical Trial.JAMA Netw Open. 2024 Mar 4;7(3):e2356445. doi: 10.1001/jamanetworkopen.2023.56445. JAMA Netw Open. 2024. PMID: 38441897 Free PMC article. Clinical Trial.
-
Clinical Outcomes After Acute Coronary Syndromes or Revascularization Among People Living With HIV: A Systematic Review and Meta-Analysis.JAMA Netw Open. 2024 May 1;7(5):e2411159. doi: 10.1001/jamanetworkopen.2024.11159. JAMA Netw Open. 2024. PMID: 38743421 Free PMC article.
-
Virtual adaptation of a nurse-driven strategy to improve blood pressure control among people with HIV.HIV Res Clin Pract. 2025 Dec;26(1):2477396. doi: 10.1080/25787489.2025.2477396. Epub 2025 Mar 18. HIV Res Clin Pract. 2025. PMID: 40099639
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
