

Invasive coronary physiology in patients with angina and non-obstructive coronary artery disease: a consensus document from the coronary microvascular dysfunction workstream of the British Heart Foundation/National Institute for Health Research Partnership
- PMID: 35318254
- PMCID: PMC9811089
- DOI: 10.1136/heartjnl-2021-320718
Invasive coronary physiology in patients with angina and non-obstructive coronary artery disease: a consensus document from the coronary microvascular dysfunction workstream of the British Heart Foundation/National Institute for Health Research Partnership
Abstract
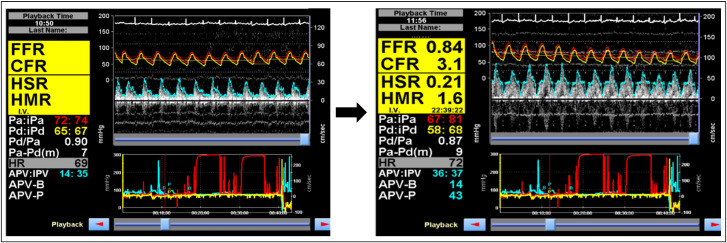
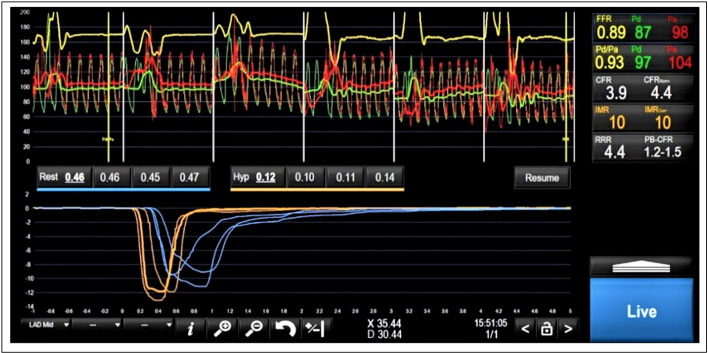
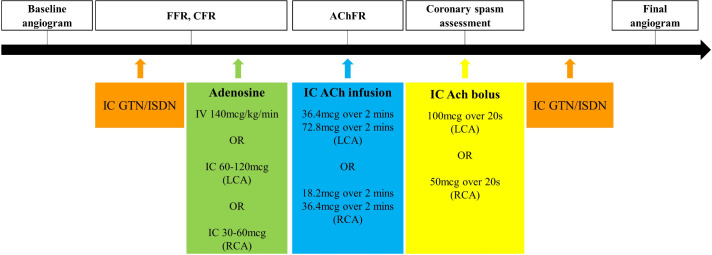
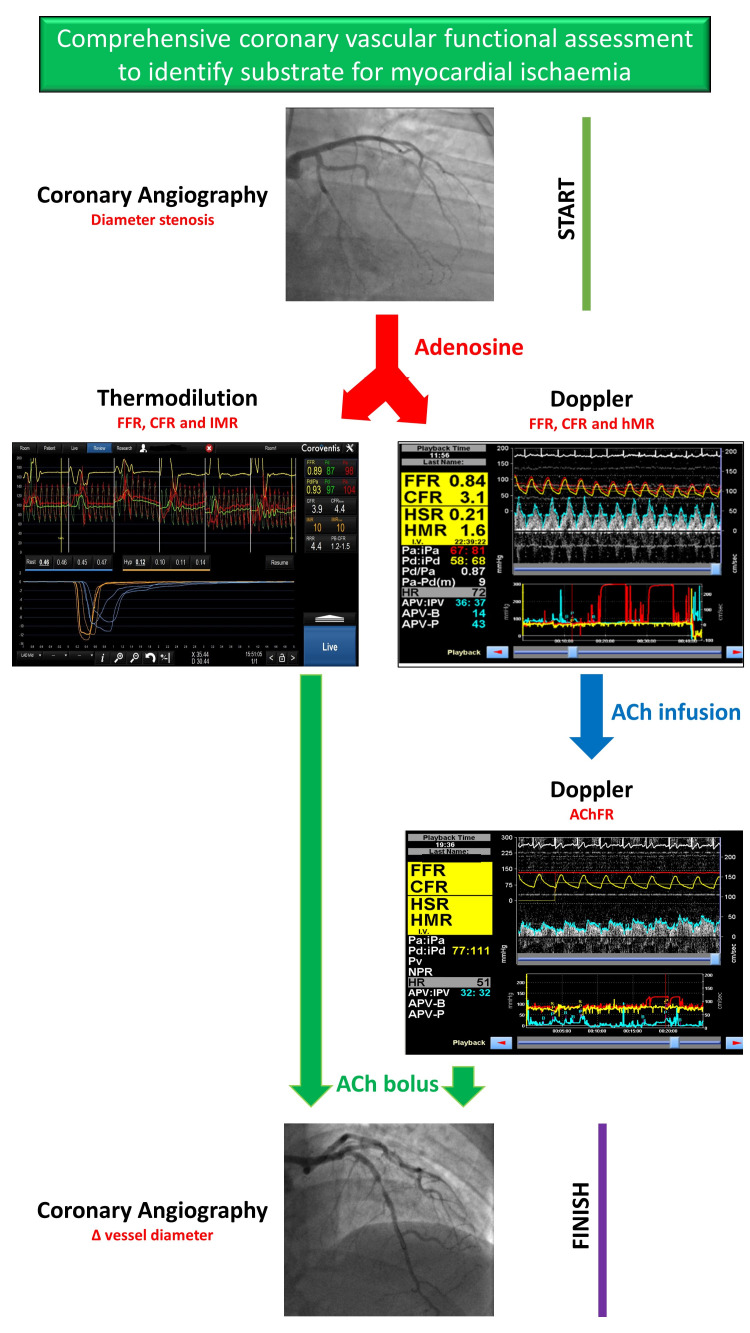
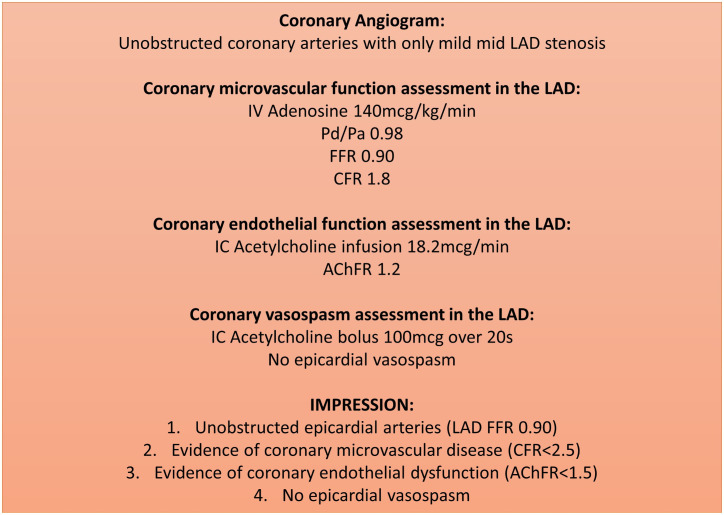
Nearly half of all patients with angina have non-obstructive coronary artery disease (ANOCA); this is an umbrella term comprising heterogeneous vascular disorders, each with disparate pathophysiology and prognosis. Approximately two-thirds of patients with ANOCA have coronary microvascular disease (CMD). CMD can be secondary to architectural changes within the microcirculation or secondary to vasomotor dysfunction. An inability of the coronary vasculature to augment blood flow in response to heightened myocardial demand is defined as an impaired coronary flow reserve (CFR), which can be measured non-invasively, using imaging, or invasively during cardiac catheterisation. Impaired CFR is associated with myocardial ischaemia and adverse cardiovascular outcomes.The CMD workstream is part of the cardiovascular partnership between the British Heart Foundation and The National Institute for Health Research in the UK and comprises specialist cardiac centres with expertise in coronary physiology assessment. This document outlines the two main modalities (thermodilution and Doppler techniques) for estimation of coronary flow, vasomotor testing using acetylcholine, and outlines a standard operating procedure that could be considered for adoption by national networks. Accurate and timely disease characterisation of patients with ANOCA will enable clinicians to tailor therapy according to their patients' coronary physiology. This has been shown to improve patients' quality of life and may lead to improved cardiovascular outcomes in the long term.
Keywords: Angina Pectoris; Chest Pain; Coronary Angiography; Microvascular Angina.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: DP has received support for a research grant from Abbott Vascular and Philips Volcano in the past. CB is employed by The University of Glasgow, which holds research and consultancy agreements for work done in the course of his employment with the following companies: AstraZeneca, Abbott Vascular, GSK, Heartflow, Menarini, Novartis, Philips and Siemens Healthcare. PDM has received speaker’s honoraria from Abbott Vascular. RP has received speaker’s honoraria from Philips Volcano.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical