

Dimensions and forms of artefacts in 1.5 T and 3 T MRI caused by cochlear implants
- PMID: 35318407
- PMCID: PMC8940987
- DOI: 10.1038/s41598-022-08988-2
Dimensions and forms of artefacts in 1.5 T and 3 T MRI caused by cochlear implants
Abstract
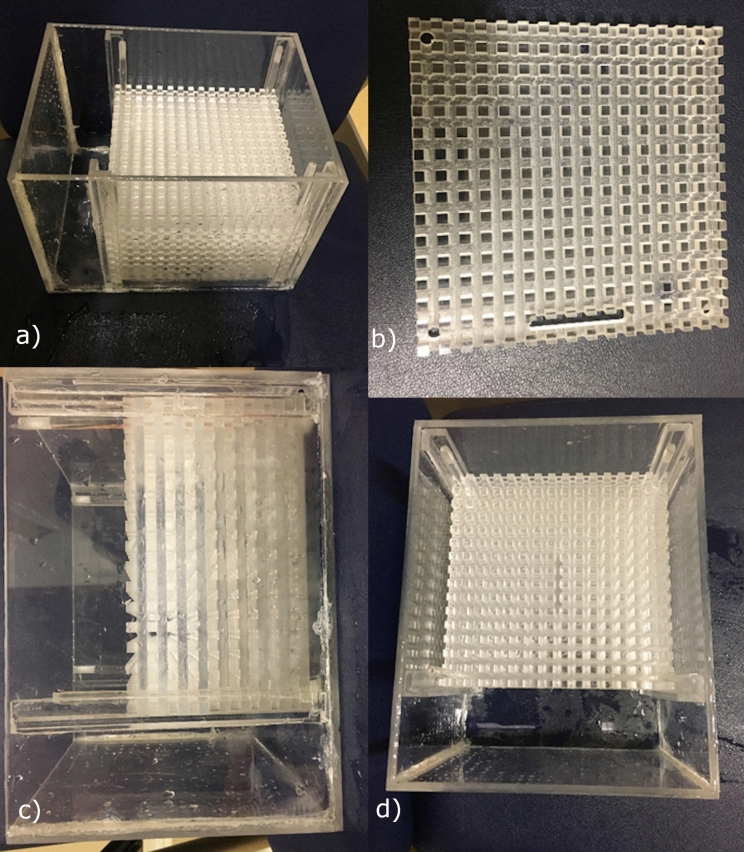
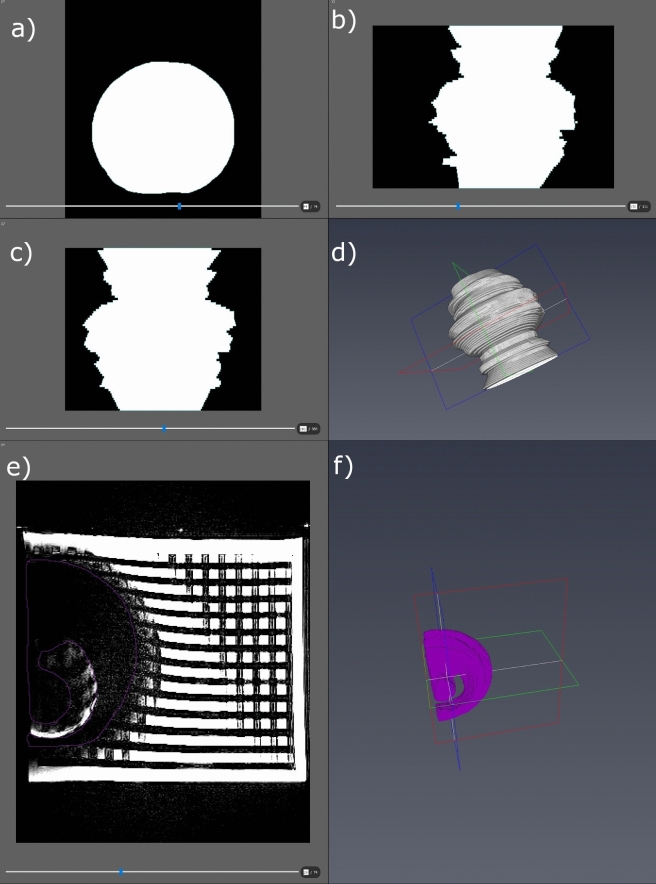
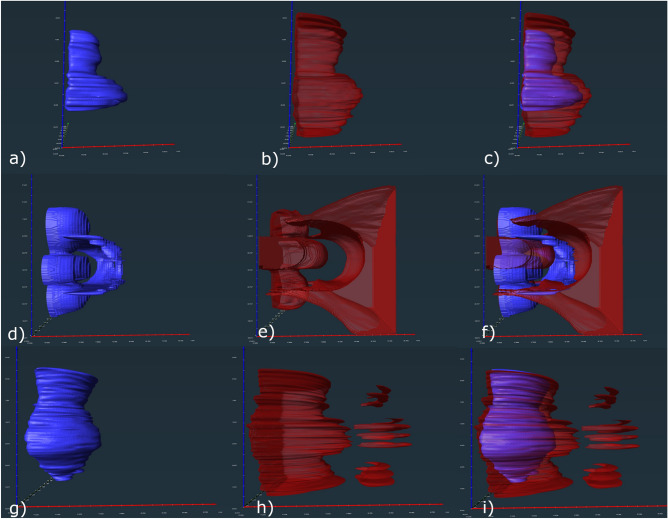
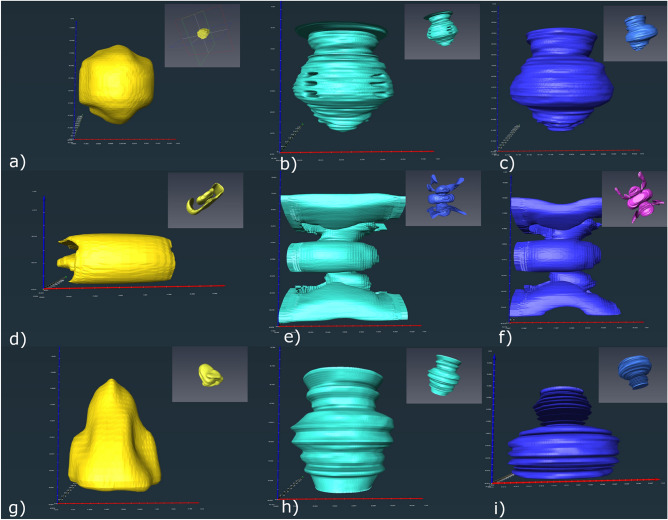
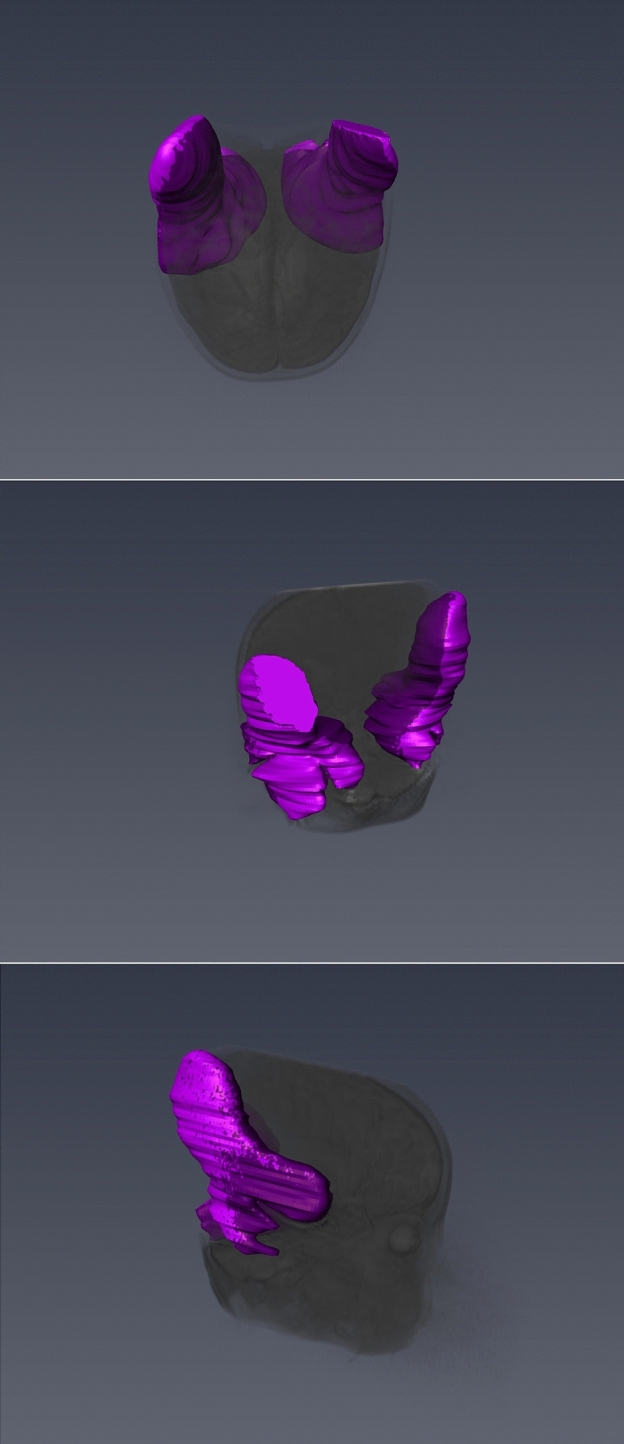
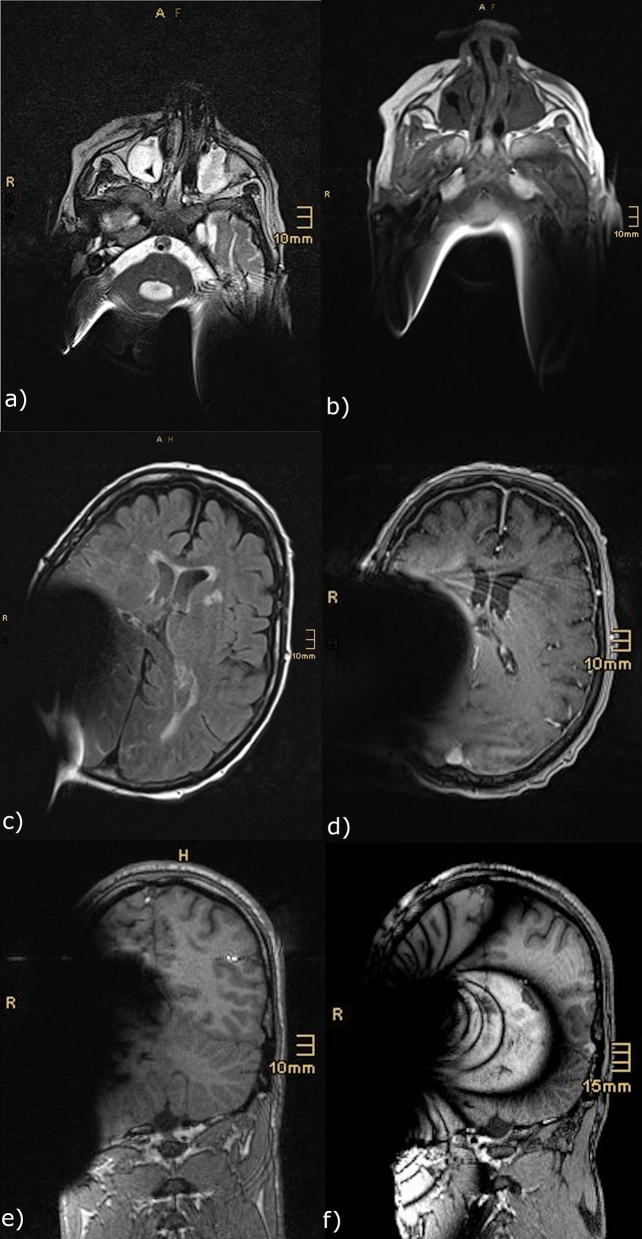
Cochlear implantation is a standard treatment option due to expanding indications. Cranial magnetic resonance imaging (cMRI) has become a widespread diagnostic tool. Therefore, an increased number of cochlear implant (CI) users are undergoing cMRI scans. This study aimed to investigate the issue of the CI magnet impacting MRI quality and artifacts. 1.5 T and 3 T MRI scans with 4 defined sequences (T2-TSE, T2-TIRM, T1-3D-MPRAGE, and TDI) were performed on a phantom with a CI (SYNCHRONY System by MED-EL Austria) in place. The resulting MRI artifacts were retrospectively compared to MRI artifacts observed in patients with a CI. All images were transferred to AMIRA and visualized by manual segmentation. Usable image quality was achieved in three sequences (T2-TSE, T2-TIRM and T1-mprage). Observed artifacts differed in shape and size depending on the sequence. Maximum diameters of signal void areas ranged from 58 × 108 × 98 mm to 127 × 123 × 153 mm. Image distortions were larger. MRI artifacts caused by the SYNCHRONY system are asymmetric with varying shape, depending on the sequence. The phantom artefacts are similar to those in CI users. Considering the observed asymmetry, the hypothesis of varying implantation locations resulting in varying positions of the signal void area needs to be further investigated.
© 2022. The Author(s).
Conflict of interest statement
The corresponding author received research funds from the the R&D Department of MED-EL Elektromedizinische Geräte GmbH Innsbruck.
Figures
References
-
- US Department of Health & Human Services NIoDaoCD. Cochlear Implants. (2017).
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
