

Remdesivir use and risks of acute kidney injury and acute liver injury among patients hospitalised with COVID-19: a self-controlled case series study
- PMID: 35318694
- PMCID: PMC9111503
- DOI: 10.1111/apt.16894
Remdesivir use and risks of acute kidney injury and acute liver injury among patients hospitalised with COVID-19: a self-controlled case series study
Abstract
Background and aim: To investigate and quantify the risks of AKI and ALI associated with remdesivir use, given the underlying diseases of SARS-CoV-2 infection.
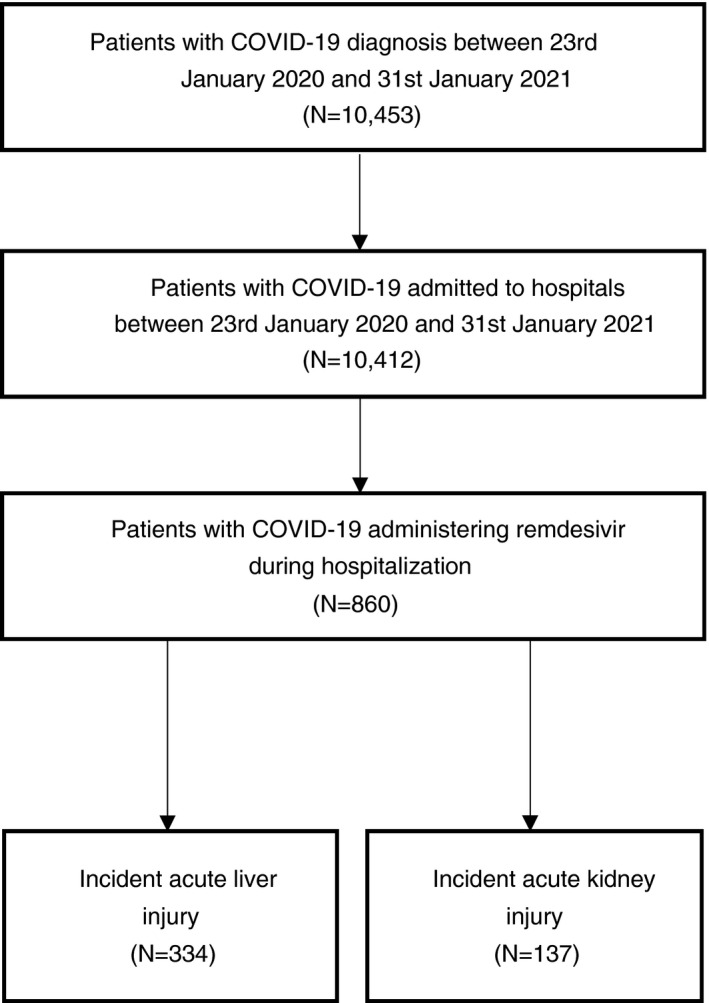
Methods: This self-controlled case series (SCCS) study was conducted using electronic hospital records between 23 January 2020 and 31 January 2021 as retrieved from the Hong Kong Hospital Authority which manages all laboratory-confirmed COVID-19 cases in Hong Kong. Outcomes of AKI and ALI were defined using the KDIGO Guideline and Asia Pacific Association of Study of Liver consensus guidelines. Incidence rate ratios (IRR) for AKI and ALI following the administration of remdesivir (exposure) in comparison to a non-exposure period were estimated using the conditional Poisson regression models.
Results: Of 860 COVID-19 patients administered remdesivir during hospitalisation, 334 (38.8%) and 137 (15.9%) had incident ALI and AKI, respectively. Compared with the baseline period, both ALI and AKI risks were increased significantly during the pre-exposure period (ALI: IRR = 6.169, 95% CI = 4.549-8.365; AKI: IRR = 7.074, 95% CI = 3.763-13.298) and remained elevated during remdesivir treatment. Compared to the pre-exposure period, risks of ALI and AKI were not significantly higher in the first 2 days of remdesivir initiation (ALI: IRR = 1.261, 95% CI = 0.915-1.737; AKI: IRR = 1.261, 95% CI = 0.889-1.789) and between days 2 and 5 of remdesivir treatment (ALI: IRR = 1.087, 95% CI = 0.793-1.489; AKI: IRR = 1.152, 95% CI = 0.821-1.616).
Conclusion: The increased risks of AKI and ALI associated with intravenous remdesivir treatment for COVID-19 may be due to the underlying SARS-CoV-2 infection. The risks of AKI and ALI were elevated in the pre-exposure period, yet no such increased risks were observed following remdesivir initiation when compared to the pre-exposure period.
Keywords: COVID-19; acute kidney injury; acute liver injury; case series; remdesivir.
© 2022 John Wiley & Sons Ltd.
Figures

Comment in
-
Editorial: liver and kidney injury from remdesivir-an issue not as much as its purpose. Authors' reply.Aliment Pharmacol Ther. 2022 Jun;55(11):1457-1458. doi: 10.1111/apt.16932. Aliment Pharmacol Ther. 2022. PMID: 35538354 No abstract available.
-
Editorial: liver and kidney injury from remdesivir-an issue not as much as its purpose.Aliment Pharmacol Ther. 2022 Jun;55(11):1456. doi: 10.1111/apt.16921. Aliment Pharmacol Ther. 2022. PMID: 35538355 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous