

Bifurcation occlusions and endovascular treatment outcome in acute ischemic stroke
- PMID: 35318957
- PMCID: PMC10086510
- DOI: 10.1136/neurintsurg-2021-018560
Bifurcation occlusions and endovascular treatment outcome in acute ischemic stroke
Abstract
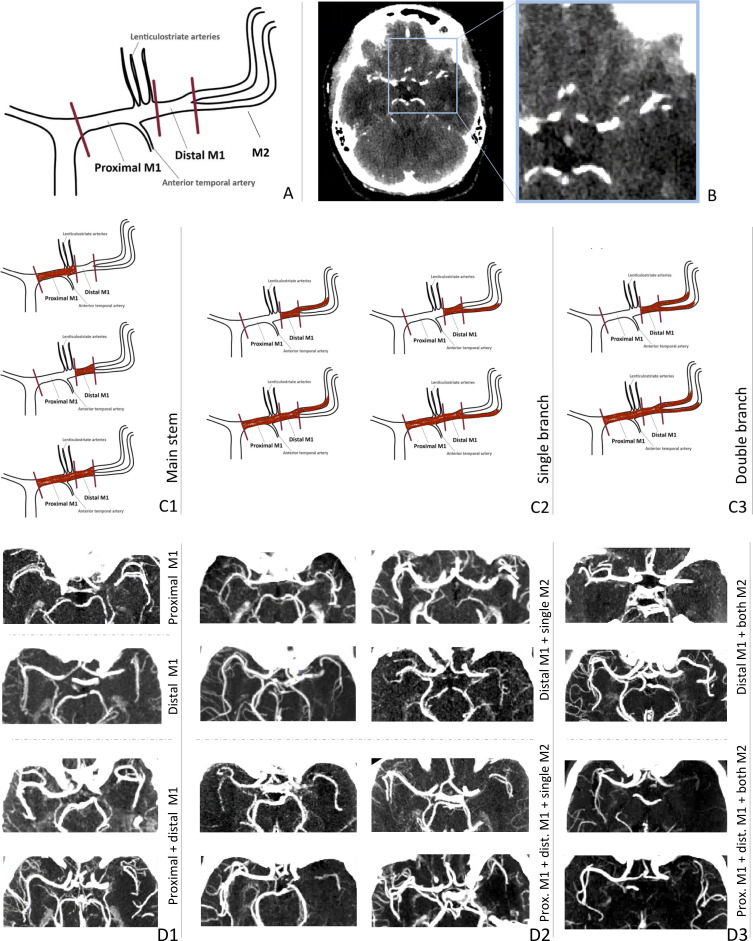
Background: A thrombus in the M1 segment of the middle cerebral artery (MCA) can occlude this main stem only or extend into the M1-M2 bifurcation. The occlusion pattern may affect endovascular treatment (EVT) success, as a bifurcated thrombus may be more prone to fragmentation during retrieval.
Objective: To investigate whether bifurcated thrombus patterns are associated with EVT procedural and clinical outcomes.
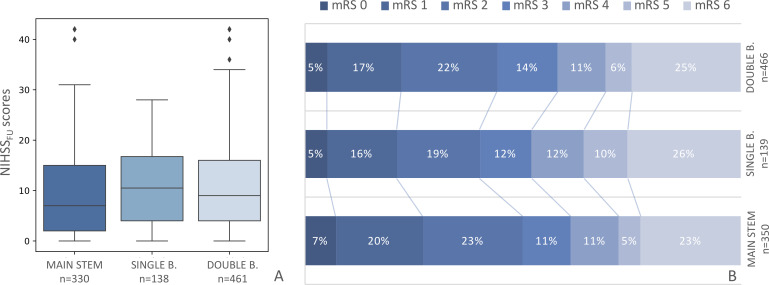
Methods: Occlusion patterns of MCA thrombi on CT angiography from MR CLEAN Registry patients were classified into three groups: main stem occlusion, bifurcation occlusion extending into one M2 branch, and bifurcation occlusion extending into both M2 branches. Procedural parameters, procedural outcomes (reperfusion grade and embolization to new territory), and clinical outcomes (24-48 hour National Institutes of Health Stroke Scale [NIHSSFU] score, change in NIHSS scores between 24 and 48 hours and baseline ∆ [NIHSS], and 90-day modified Rankin Scale [mRS] scores) were compared between occlusion patterns.
Results: We identified 1023 patients with an MCA occlusion of whom 370 (36%) had a main stem occlusion, 151 (15%) a single branch, and 502 (49%) a double branch bifurcation occlusion. There were no statistically significant differences in retrieval method, procedure time, number of retrieval attempts, reperfusion grade, and embolization to new territory between occlusion patterns. Patients with main stem occlusions had lower NIHSSFU scores than patients with single (7 vs 11, p=0.01) or double branch occlusions (7 vs 9, p=0.04). However, there were no statistically significant differences in ∆ NIHSS or in 90-day mRS scores.
Conclusions: In our population, EVT procedural and long-term clinical outcomes were similar for MCA bifurcation occlusions and MCA main stem occlusions.
Keywords: CT Angiography; Stent; Stroke; Thrombectomy.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: This project has received funding from the European Union’s Horizon 2020 research and innovation program under grant agreement No 777072 (INSIST project), and the AMC medical Research BV, Amsterdam UMC, location AMC, under project No 21937. The MR CLEAN registry is partially funded by unrestricted grants from the Applied Scientific Institute for Neuromodulation (Toegepast Wetenschappelijk Instituut voor Neuromodulatie), Erasmus Medical Center, Amsterdam University Medical Center and Maastricht University Medical Center. HAM reports co-founder and shareholder of Nicolab, a company that focuses on the use of artificial intelligence for medical image analysis. CBLMM reports grants from European Commission during the conduct of the study; grants from CVON/Dutch Heart Foundation, TWIN Foundation, and Stryker, outside the submitted work; and shareholder of Nicolab. IGHJ reports shareholder of Nicolab. DWJD and AvdL report unrestricted grants from Stryker, Penumbra, Medtronic, Cerenovus, Thrombolytic Science, LLC, Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organization for Health Research and Development, Health Holland Top Sector Life Sciences and Health, and Thrombolytic Science, LLC for research, paid to institution. BvdW received funds from Bayer and LivaNova for consultancy, paid to his institution, and grants from the Dutch Heart Foundation, the Horizon 2020 programme, and Stryker, paid to his institution, all outside the work submitted. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical