

Update on the clinical management of multiple endocrine neoplasia type 1
- PMID: 35319130
- PMCID: PMC9540817
- DOI: 10.1111/cen.14727
Update on the clinical management of multiple endocrine neoplasia type 1
Abstract
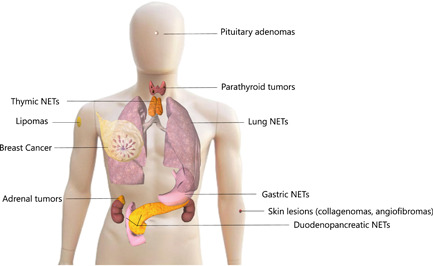
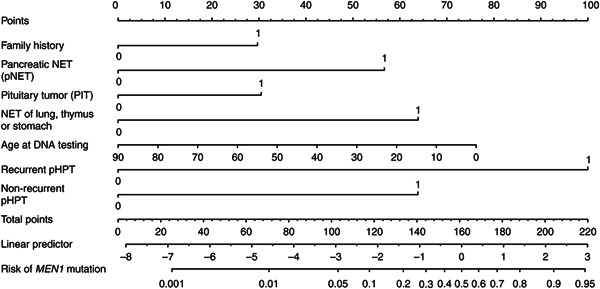
This review provides an overview of novel insights in the clinical management of patients with Multiple Endocrine Neoplasia Type 1, focusing on the last decade since the last update of the MEN1 guidelines. With regard to Diagnosis: Mutation-negative patients with 2/3 main manifestations have a different clinical course compared to mutation-positive patients. As for primary hyperparathyroidism: subtotal parathyroidectomy is the initial procedure of choice. Current debate centres around the timing of initial parathyroidectomy as well as the controversial topic of unilateral clearance in young patients. For duodenopancreatic neuroendocrine tumours (NETs), the main challenge is accurate and individualized risk stratification to enable personalized surveillance and treatment. Thymus NETs remain one of the most aggressive MEN1-related tumours. Lung NETs are more frequent than previously thought, generally indolent, but rare aggressive cases do occur. Pituitary adenomas are most often prolactinomas and nonfunctioning microadenomas with an excellent prognosis and good response to therapy. Breast cancer is recognized as part of the MEN1 syndrome in women and periodical screening is advised. Clinically relevant manifestations are already seen at the paediatric age and initiating screening in the second decade is advisable. MEN1 has a significant impact on quality of life and US data show a significant financial burden. In conclusion, patient outcomes have improved, but much is still to be achieved. For care tailored to the needs of the individual patient and improving outcomes on an individual basis, studies are now needed to define predictors of tumour behaviour and effects of more individualized interventions.
Keywords: disease management; genetic testing; multiple endocrine neoplasia type 1; neuroendocrine tumours; pituitary neoplasms; primary hyperparathyroidism; review.
© 2022 The Authors. Clinical Endocrinology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Chandrasekharappa SC, Guru SC, Manickam P, et al. Positional cloning of the gene for multiple endocrine neoplasia‐type 1. Science. 1997;276:404‐407. - PubMed
-
- Thakker RV, Newey PJ, Walls GV, et al. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1). J Clin Endocrinol Metab. 2012;97(9):2990‐3011. - PubMed
-
- Romanet P, Mohamed A, Giraud S, et al. UMD‐MEN1 Database: an overview of the 370 MEN1 variants present in 1676 patients from the French population. J Clin Endocrinol Metab. 2019;104(3):753‐764. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
