

Mechanism of injury and special considerations as predictive of serious injury: A systematic review
- PMID: 35319149
- PMCID: PMC9545392
- DOI: 10.1111/acem.14489
Mechanism of injury and special considerations as predictive of serious injury: A systematic review
Abstract
Objectives: The Centers for Disease Control and Prevention's field triage guidelines (FTG) are routinely used by emergency medical services personnel for triaging injured patients. The most recent (2011) FTG contains physiologic, anatomic, mechanism, and special consideration steps. Our objective was to systematically review the criteria in the mechanism and special consideration steps that might be predictive of serious injury or need for a trauma center.
Methods: We conducted a systematic review of the predictive utility of mechanism and special consideration criteria for predicting serious injury. A research librarian searched in Ovid Medline, EMBASE, and the Cochrane databases for studies published between January 2011 and February 2021. Eligible studies were identified using a priori inclusion and exclusion criteria. Studies were excluded if they lacked an outcome for serious injury, such as measures of resource use, injury severity scores, mortality, or composite measures using a combination of outcomes. Given the heterogeneity in populations, measures, and outcomes, results were synthesized qualitatively focusing on positive likelihood ratios (LR+) whenever these could be calculated from presented data or adjusted odds ratios (aOR).
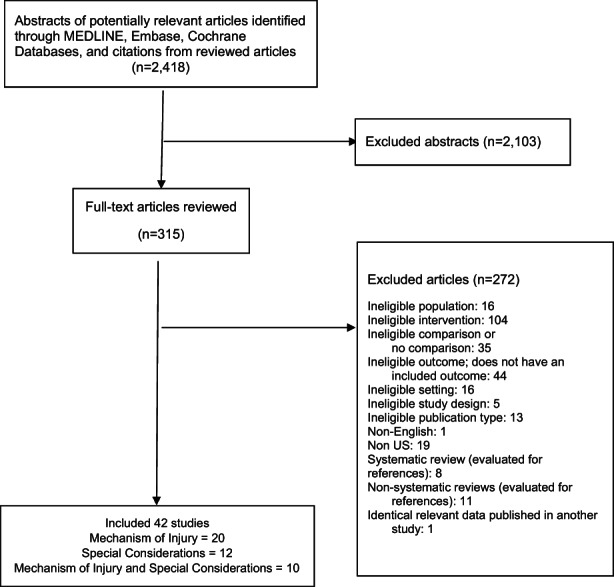
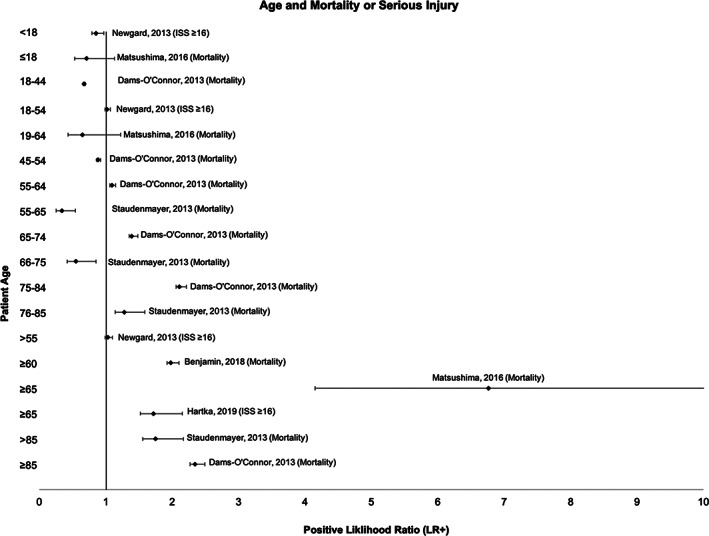
Results: We reviewed 2418 abstracts and 315 full-text publications and identified 42 relevant studies. The factors most predictive of serious injury across multiple studies were death in the same vehicle (LR+ 2.2-7.4), ejection (aOR 3.2-266.2), extrication (LR+ 1.1-6.6), lack of seat belt use (aOR 4.4-11.3), high speeds (aOR 2.0-2.9), concerning crash variables identified by vehicle telemetry systems (LR+ 4.7-22.2), falls from height (LR+ 2.4-5.9), and axial load or diving (aOR 2.5-17.6). Minor or inconsistent predictors of serious injury were vehicle intrusion (LR+ 0.8-7.2), cardiopulmonary or neurologic comorbidities (LR+ 0.8-3.1), older age (LR+ 0.6-6.8), or anticoagulant use (LR+ 1.1-1.8).
Conclusions: Select mechanism and special consideration criteria contribute positively to appropriate field triage of potentially injured patients.
Keywords: age; emergency medical services; field triage; field triage guidelines; mechanism of injury; prehospital care; serious injury; special considerations; trauma.
© 2022 The Authors. Academic Emergency Medicine published by Wiley Periodicals LLC on behalf of Society for Academic Emergency Medicine.
Conflict of interest statement
All authors report no conflict of interest.
Figures
References
-
- Sasser SM, Hunt RC, Faul M, et al. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR Recomm Rep. 2012;61(RR‐1):1‐20. - PubMed
-
- Sasser SM, Hunt RC, Sullivent EE, et al. Guidelines for field triage of injured patients. Recommendations of the National Expert Panel on Field Triage. MMWR Recomm Rep 2009;58(RR‐1):1–35. - PubMed
