

Multiple Routes of Antibody-Dependent Enhancement of SARS-CoV-2 Infection
- PMID: 35319248
- PMCID: PMC9045191
- DOI: 10.1128/spectrum.01553-21
Multiple Routes of Antibody-Dependent Enhancement of SARS-CoV-2 Infection
Abstract
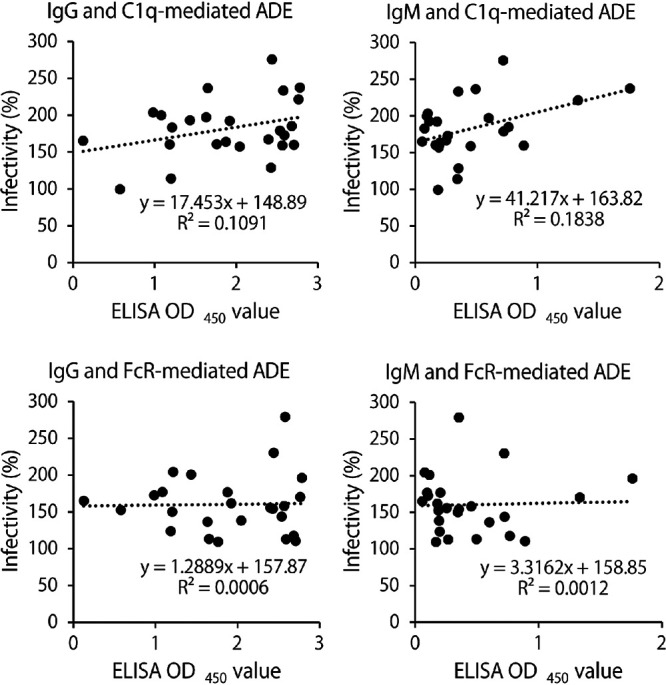
Antibody-dependent enhancement (ADE) of infection is generally known for many viruses. A potential risk of ADE in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has also been discussed since the beginning of the coronavirus disease 2019 (COVID-19) pandemic; however, clinical evidence of the presence of antibodies with ADE potential is limited. Here, we show that ADE antibodies are produced by SARS-CoV-2 infection and the ADE process can be mediated by at least two different host factors, Fcγ receptor (FcγR) and complement component C1q. Of 89 serum samples collected from acute or convalescent COVID-19 patients, 62.9% were found to be positive for SARS-CoV-2-specific IgG. FcγR- and/or C1q-mediated ADE were detected in 50% of the IgG-positive sera, whereas most of them showed neutralizing activity in the absence of FcγR and C1q. Importantly, ADE antibodies were found in 41.4% of the acute COVID-19 patients. Neutralizing activity was also detected in most of the IgG-positive sera, but it was counteracted by ADE in subneutralizing conditions in the presence of FcγR or C1q. Although the clinical importance of ADE needs to be further investigated with larger numbers of COVID-19 patient samples, our data suggest that SARS-CoV-2 utilizes multiple mechanisms of ADE. C1q-mediated ADE may particularly have a clinical impact since C1q is present at high concentrations in plasma and its receptors are ubiquitously expressed on the surfaces of many types of cells, including respiratory epithelial cells, which SARS-CoV-2 primarily infects. IMPORTANCE Potential risks of antibody-dependent enhancement (ADE) in the coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection has been discussed and the proposed mechanism mostly depends on the Fc gamma receptor (FcγR). However, since FcγRs are exclusively expressed on immune cells, which are not primary targets of SARS-CoV-2, the clinical importance of ADE of SARS-CoV-2 infection remains controversial. Our study demonstrates that SARS-CoV-2 infection induces antibodies that increase SARS-CoV-2 infection through another ADE mechanism in which complement component C1q mediates the enhancement. Although neutralizing activity was also detected in the serum samples, it was counteracted by ADE in the presence of FcγR or C1q. Considering the ubiquity of C1q and its cellular receptors, C1q-mediated ADE may more likely occur in respiratory epithelial cells, which SARS-CoV-2 primarily infects. Our data highlight the importance of careful monitoring of the antibody properties in COVID-19 convalescent and vaccinated individuals.
Keywords: ADE; C1q; COVID-19; Fc receptor; FcR; SARS-CoV-2; antibody-dependent enhancement; complement.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






Similar articles
-
Antibody-Dependent Enhancement of SARS-CoV-2 Infection Is Mediated by the IgG Receptors FcγRIIA and FcγRIIIA but Does Not Contribute to Aberrant Cytokine Production by Macrophages.mBio. 2021 Oct 26;12(5):e0198721. doi: 10.1128/mBio.01987-21. Epub 2021 Sep 28. mBio. 2021. PMID: 34579572 Free PMC article.
-
Antibody-Dependent Enhancement (ADE) and the role of complement system in disease pathogenesis.Mol Immunol. 2022 Dec;152:172-182. doi: 10.1016/j.molimm.2022.11.010. Epub 2022 Nov 10. Mol Immunol. 2022. PMID: 36371813 Free PMC article. Review.
-
Antibody-dependent enhancement of SARS-CoV-2, the impact of variants and vaccination.Hum Vaccin Immunother. 2025 Dec;21(1):2505356. doi: 10.1080/21645515.2025.2505356. Epub 2025 May 24. Hum Vaccin Immunother. 2025. PMID: 40411306 Free PMC article.
-
The role of IgG Fc receptors in antibody-dependent enhancement.Nat Rev Immunol. 2020 Oct;20(10):633-643. doi: 10.1038/s41577-020-00410-0. Epub 2020 Aug 11. Nat Rev Immunol. 2020. PMID: 32782358 Free PMC article. Review.
-
Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies.Front Immunol. 2021 Feb 24;12:640093. doi: 10.3389/fimmu.2021.640093. eCollection 2021. Front Immunol. 2021. PMID: 33717193 Free PMC article.
Cited by
-
The interplay between previous infection and mental health condition on antibody response to COVID-19 mRNA vaccination.Brain Behav Immun Health. 2023 Aug 25;33:100677. doi: 10.1016/j.bbih.2023.100677. eCollection 2023 Nov. Brain Behav Immun Health. 2023. PMID: 37701787 Free PMC article.
-
Parameter identifiability of a within-host SARS-CoV-2 epidemic model.Infect Dis Model. 2024 May 14;9(3):975-994. doi: 10.1016/j.idm.2024.05.004. eCollection 2024 Sep. Infect Dis Model. 2024. PMID: 38881537 Free PMC article.
-
The Role of Antibodies in the Treatment of SARS-CoV-2 Virus Infection, and Evaluating Their Contribution to Antibody-Dependent Enhancement of Infection.Int J Mol Sci. 2022 May 28;23(11):6078. doi: 10.3390/ijms23116078. Int J Mol Sci. 2022. PMID: 35682757 Free PMC article. Review.
-
Antibody-dependent enhancement of coronaviruses.Int J Biol Sci. 2025 Feb 3;21(4):1686-1704. doi: 10.7150/ijbs.96112. eCollection 2025. Int J Biol Sci. 2025. PMID: 39990674 Free PMC article. Review.
-
Pulmonary function and comparative SARS-CoV-2 RBD-specific IgG antibody response among the COVID-19 recovered group.PLoS One. 2025 Jul 11;20(7):e0318959. doi: 10.1371/journal.pone.0318959. eCollection 2025. PLoS One. 2025. PMID: 40644485 Free PMC article.
References
-
- Zost SJ, Gilchuk P, Case JB, Binshtein E, Chen RE, Nkolola JP, Schäfer A, Reidy JX, Trivette A, Nargi RS, Sutton RE, Suryadevara N, Martinez D, Williamson LE, Chen EC, Jones T, Day S, Myers L, Hassan AO, Kafai NM, Winkler ES, Fox JM, Shrihari S, Mueller BK, Meiler J, Chandrashekar A, Mercado NB, Steinhardt JJ, Ren K, Loo YM, Kallewaard NL, McCune BT, Keeler SP, Holtzman MJ, Barouch DH, Gralinski LE, Baric RS, Thackray LB, Diamond MS, Carnaha RH, Crowe JE. Jr.. 2020. Potently neutralizing and protective human antibodies against SARS-CoV-2. Nature 584:443–449. doi:10.1038/s41586-020-2548-6. - DOI - PMC - PubMed
-
- Shi R, Shan C, Duan X, Chen Z, Liu P, Song J, Song T, Bi X, Han C, Wu L, Gao G, Hu X, Zhang Y, Tong Z, Huang W, Liu WJ, Wu G, Zhang B, Wang L, Qi J, Feng H, Wang F-S, Wang Q, Gao GF, Yuan Z, Yan J. 2020. A human neutralizing antibody targets the receptor-binding site of SARS-CoV-2. Nature 584:120–124. doi:10.1038/s41586-020-2381-y. - DOI - PubMed
-
- Wheatley AK, Juno JA, Wang JJ, Selva KJ, Reynaldi A, Tan HX, Lee WS, Wragg KM, Kelly HG, Esterbauer R, Davis SK, Kent HE, Mordant FL, Schlub TE, Gordon DL, Khoury DS, Subbarao K, Cromer D, Gordon TP, Chung AW, Davenport MP, Kent SJ. 2021. Evolution of immune responses to SARS-CoV-2 in mild-moderate COVID-19. Nat Commun 12:1162. doi:10.1038/s41467-021-21444-5. - DOI - PMC - PubMed
-
- Gerhards C, Thiaucourt M, Kittel M, Becker C, Ast V, Hetjens M, Neumaier M, Haselmann V. 2021. Longitudinal assessment of anti-SARS-CoV-2 antibody dynamics and clinical features following convalescent from COVID-19 infection. Int J Infect Dis 107:221–227. doi:10.1016/j.ijid.2021.04.080. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
