

Corticotroph pituitary carcinoma with skeletal metastases masquerading as ectopic ACTH syndrome: a long and winding road to diagnosis
- PMID: 35319488
- PMCID: PMC9002182
- DOI: 10.1530/EDM-21-0168
Corticotroph pituitary carcinoma with skeletal metastases masquerading as ectopic ACTH syndrome: a long and winding road to diagnosis
Abstract
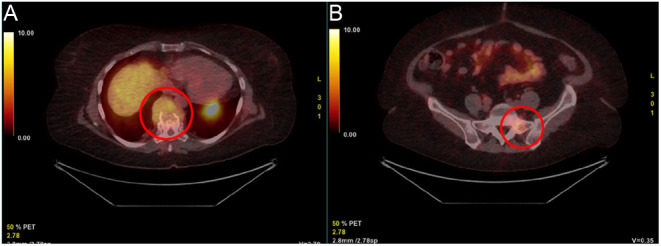
Summary: Pituitary carcinoma is a rare type of malignancy and only accounts for 0.1-0.2% of all pituitary tumours. Most pituitary carcinomas are hormonally active and they are mostly represented by corticotroph and lactotroph carcinomas. Corticotroph carcinoma can present as symptomatic Cushing's disease or can evolve from silent corticotroph adenoma which is not associated with clinical or biochemical evidence of hypercortisolism. We hereby present a case of a bone-metastasized corticotroph pituitary carcinoma masquerading as an ectopic adrenocorticotropic hormone (ACTH) syndrome in a patient with a history of a non-functioning pituitary macro-adenoma. Our patient underwent two transsphenoidal resections of the primary pituitary tumour followed by external beam radiation therapy. Under hydrocortisone substitution therapy she developed ACTH-dependent hypercortisolism without arguments for recurrence on pituitary MRI and without central-to-peripheral ACTH-gradient on inferior petrosal sinus sampling, both suggesting ectopic production. Ultimately, she was diagnosed with an ACTH-secreting vertebral metastasis originating from the primary pituitary tumour. This case report demonstrates the complex pathophysiology of pituitary carcinoma and the long diagnostic work-up. Certain features in pituitary adenoma should raise the suspicion of malignancy.
Learning points: The diagnosis of pituitary carcinoma can only be made based on documented metastasis, therefore, due to the often long latency period between the detection of the primary tumour and the occurrence of metastasis, the diagnostic work-up most often spans over multiple years. Pituitary carcinoma including corticotroph carcinoma is very rare in contrast to pituitary adenoma and only accounts for 0.1-0.2% of all pituitary tumours. Histopathology in pituitary adenoma should certainly accomplish the following goals: accurate tumour subtyping and assessment of tumoural proliferative potential. Repeated recurrence of pituitary adenoma after surgical resection, a discrepancy between biochemical and radiological findings, resistance to medical and radiation therapy, and silent tumours becoming functional are all hallmarks of pituitary carcinoma. Silent corticotroph adenomas are non-functioning pituitary adenomas that arise from T-PIT lineage adenohypophyseal cells and that can express adrenocorticotropic hormone on immunohistochemistry, but are not associated with biochemical or clinical evidence of hypercortisolism. Silent corticotroph adenomas exhibit a more aggressive clinical behaviour than other non-functioning adenomas. Treatment options for corticotroph carcinoma include primary tumour resection, radiation therapy, medical therapy, and chemotherapy. Sometimes bilateral adrenalectomy is necessary to achieve sufficient control of the cortisol excess.
Figures




References
LinkOut - more resources
Full Text Sources
