

Listeria delivers tetanus toxoid protein to pancreatic tumors and induces cancer cell death in mice
- PMID: 35320003
- PMCID: PMC9031812
- DOI: 10.1126/scitranslmed.abc1600
Listeria delivers tetanus toxoid protein to pancreatic tumors and induces cancer cell death in mice
Abstract
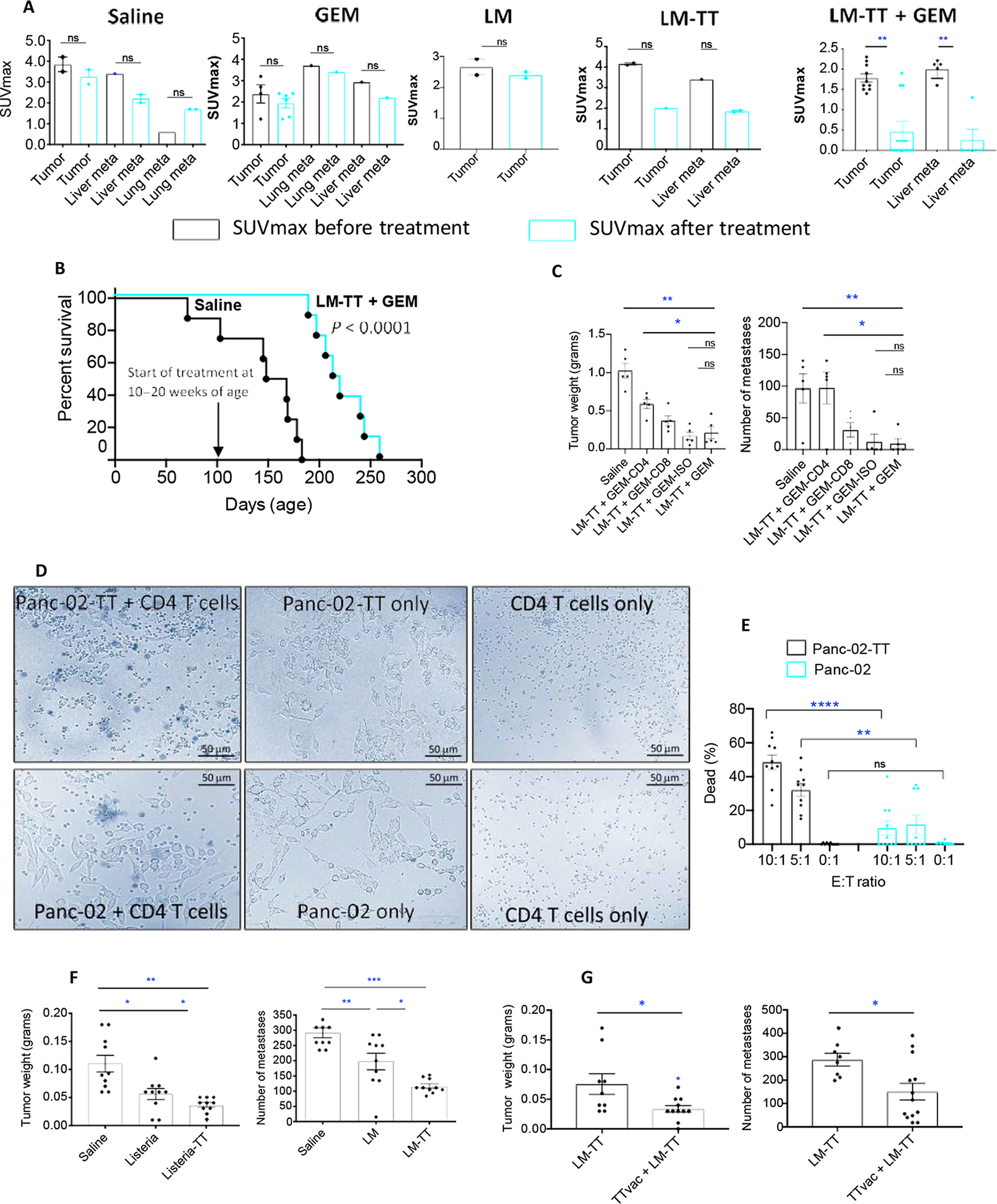
Pancreatic ductal adenocarcinoma (PDAC) is a highly metastatic disease. Tumors are poorly immunogenic and immunosuppressive, preventing T cell activation in the tumor microenvironment. Here, we present a microbial-based immunotherapeutic treatment for selective delivery of an immunogenic tetanus toxoid protein (TT856-1313) into PDAC tumor cells by attenuated Listeria monocytogenes. This treatment reactivated preexisting TT-specific memory T cells to kill infected tumor cells in mice. Treatment of KrasG12D,p53R172H, Pdx1-Cre (KPC) mice with Listeria-TT resulted in TT accumulation inside tumor cells, attraction of TT-specific memory CD4 T cells to the tumor microenvironment, and production of perforin and granzyme B in tumors. Low doses of gemcitabine (GEM) increased immune effects of Listeria-TT, turning immunologically cold into hot tumors in mice. In vivo depletion of T cells from Listeria-TT + GEM-treated mice demonstrated a CD4 T cell-mediated reduction in tumor burden. CD4 T cells from TT-vaccinated mice were able to kill TT-expressing Panc-02 tumor cells in vitro. In addition, peritumoral lymph node-like structures were observed in close contact with pancreatic tumors in KPC mice treated with Listeria-TT or Listeria-TT + GEM. These structures displayed CD4 and CD8 T cells producing perforin and granzyme B. Whereas CD4 T cells efficiently infiltrated the KPC tumors, CD8 T cells did not. Listeria-TT + GEM treatment of KPC mice with advanced PDAC reduced tumor burden by 80% and metastases by 87% after treatment and increased survival by 40% compared to nontreated mice. These results suggest that Listeria-delivered recall antigens could be an alternative to neoantigen-mediated cancer immunotherapy.
Figures





Comment in
-
Bacteria deliver the goods.Nat Rev Drug Discov. 2022 May;21(5):336. doi: 10.1038/d41573-022-00065-7. Nat Rev Drug Discov. 2022. PMID: 35393548 No abstract available.
References
-
- Kulke MH, Blaszkowsky LS, Ryan DP, Clark JW, Meyerhardt JA, Zhu AX, Enzinger PC, Kwak EL, Muzikansky A, Lawrence C, Fuchs CS, Capecitabine plus erlotinib in gemcitabine-refractory advanced pancreatic cancer. J. Clin. Oncol 25, 4787–4792 (2007). - PubMed
-
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, Campos D, Lim R, Ding K, Clark G, Voskoglou-Nomikos T, Ptasynski M, Parulekar W; National Cancer Institute of Canada Clinical Trials Group, Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A Phase III trial of the National Cancer Institute of Canada clinical trials group. J. Clin. Oncol 25, 1960–1966 (2007). - PubMed
-
- Abbruzzese JL, Grunewald R, Weeks EA, Gravel D, Adams T, Nowak B, Mineishi S, Tarassoff P, Satterlee W, Raber MN, A phase I clinical, plasma, and cellular pharmacology study of gemcitabine. J. Clin. Oncol 9, 491–498 (1991). - PubMed
-
- Von Hoff DD, Ramanathan RK, Borad MJ, Laheru DA, Smith LS, Wood TE, Korn RL, Desai N, Trieu V, Iglesias JL, Zhang H, Soon-Shiong P, Shi T, Rajeshkumar NV, Maitra A, Hidalgo M, Gemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: A phase I/II trial. J. Clin. Oncol 29, 4548–4554 (2011). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
