

Development of a national quality framework for palliative care in a mixed generalist and specialist care model: A whole-sector approach and a modified Delphi technique
- PMID: 35320315
- PMCID: PMC8942240
- DOI: 10.1371/journal.pone.0265726
Development of a national quality framework for palliative care in a mixed generalist and specialist care model: A whole-sector approach and a modified Delphi technique
Abstract
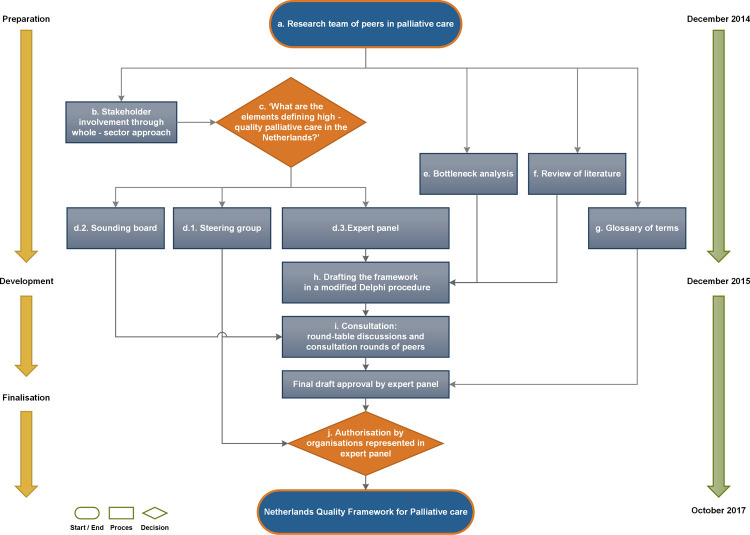
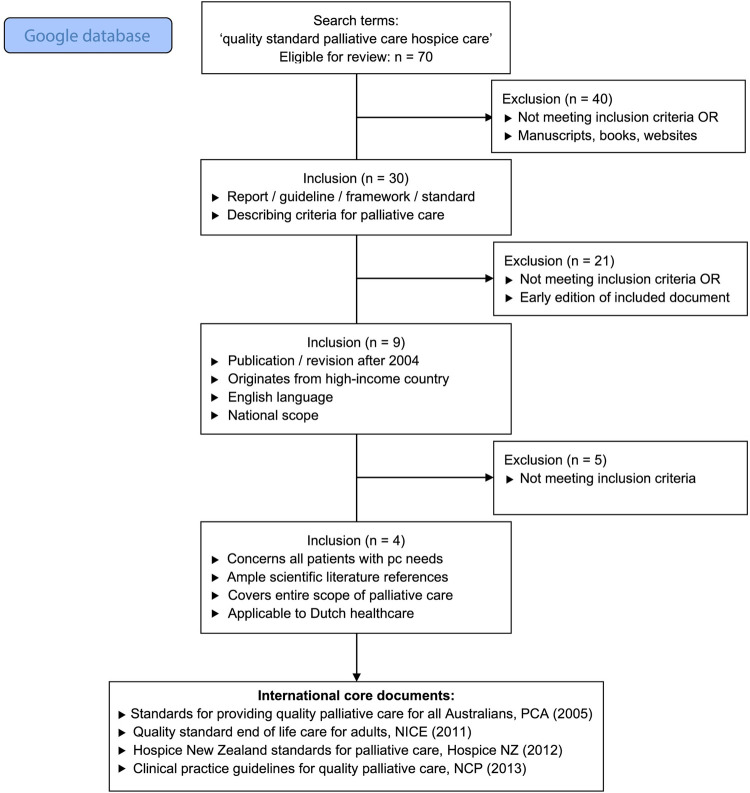
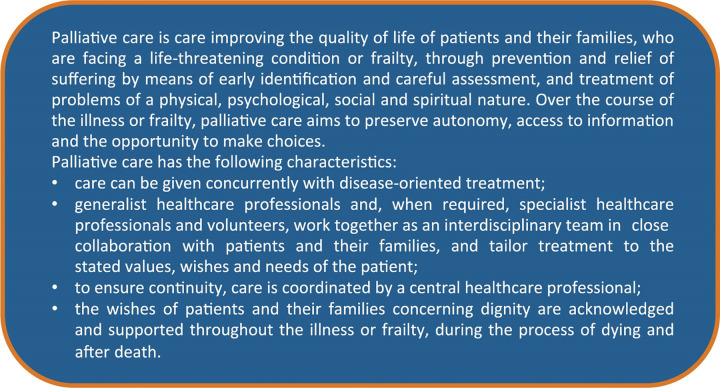
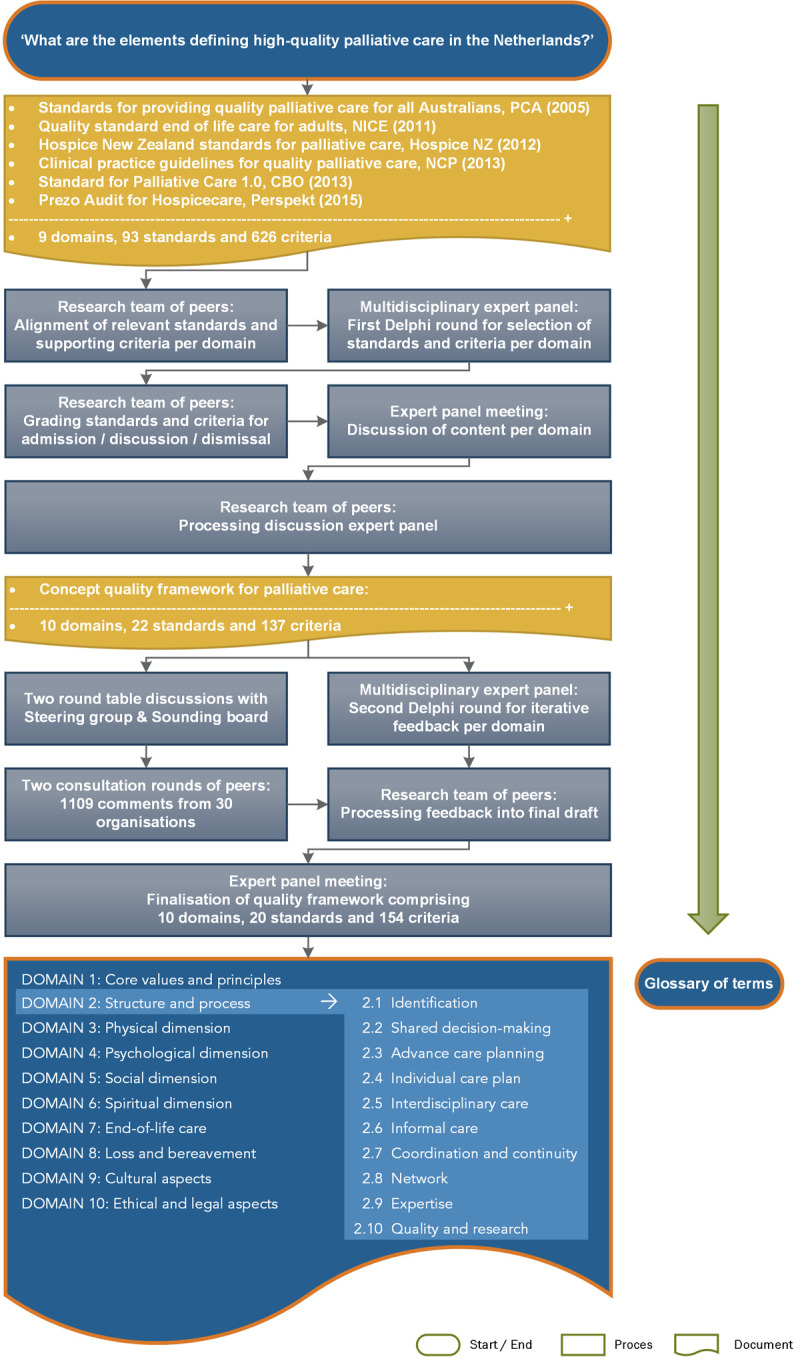
In a predominantly biomedical healthcare model focused on cure, providing optimal, person-centred palliative care is challenging. The general public, patients, and healthcare professionals are often unaware of palliative care's benefits. Poor interdisciplinary teamwork and limited communication combined with a lack of early identification of patients with palliative care needs contribute to sub-optimal palliative care provision. We aimed to develop a national quality framework to improve availability and access to high-quality palliative care in a mixed generalist-specialist palliative care model. We hypothesised that a whole-sector approach and a modified Delphi technique would be suitable to reach this aim. Analogous to the international AGREE guideline criteria and employing a whole-sector approach, an expert panel comprising mandated representatives for patients and their families, various healthcare associations, and health insurers answered the main question: 'What are the elements defining high-quality palliative care in the Netherlands?'. For constructing the quality framework, a bottleneck analysis of palliative care provision and a literature review were conducted. Six core documents were used in a modified Delphi technique to build the framework with the expert panel, while stakeholder organisations were involved and informed in round-table discussions. In the entire process, preparing and building relationships took one year and surveying, convening, discussing content, consulting peers, and obtaining final consent from all stakeholders took 18 months. A quality framework, including a glossary of terms, endorsed by organisations representing patients and their families, general practitioners, elderly care physicians, medical specialists, nurses, social workers, psychologists, spiritual caregivers, and health insurers was developed and annexed with a summary for patients and families. We successfully developed a national consensus-based patient-centred quality framework for high-quality palliative care in a mixed generalist-specialist palliative care model. A whole-sector approach and a modified Delphi technique are feasible structures to achieve this aim. The process we reported may guide other countries in their initiatives to enhance palliative care.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: CCDR declares receiving fees from Kyowa Kirin for consulting activities outside the submitted work and paid to her department. The other authors have declared that no competing interests exist. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Development of a palliative paramedicine framework to standardise best practice: A Delphi study.Palliat Med. 2024 Sep;38(8):853-873. doi: 10.1177/02692163241234004. Epub 2024 Mar 14. Palliat Med. 2024. PMID: 38483052 Free PMC article.
-
360-degree Delphi: addressing sociotechnical challenges of healthcare IT.BMC Med Inform Decis Mak. 2020 Jun 5;20(1):101. doi: 10.1186/s12911-020-1071-x. BMC Med Inform Decis Mak. 2020. PMID: 32503609 Free PMC article.
-
Identification of core indicators for the integration of a palliative care approach in hospitals: An international Delphi study.Palliat Med. 2024 Dec;38(10):1169-1183. doi: 10.1177/02692163241283540. Epub 2024 Sep 27. Palliat Med. 2024. PMID: 39340180 Free PMC article.
-
[Austrian guideline for palliative sedation therapy (long version) : Results of a Delphi process of the Austrian Palliative Society (OPG)].Wien Med Wochenschr. 2017 Feb;167(1-2):31-48. doi: 10.1007/s10354-016-0533-3. Epub 2016 Dec 6. Wien Med Wochenschr. 2017. PMID: 27924420 German.
-
Defining Core Competencies for Generalist-Level Palliative Social Work.J Pain Symptom Manage. 2018 Dec;56(6):886-892. doi: 10.1016/j.jpainsymman.2018.09.002. Epub 2018 Sep 7. J Pain Symptom Manage. 2018. PMID: 30201485
Cited by
-
Advance Care Planning: A Retrospective Audit in a National Referral Center for Interstitial Lung Diseases.Am J Hosp Palliat Care. 2025 Apr;42(4):372-381. doi: 10.1177/10499091241267914. Epub 2024 Oct 14. Am J Hosp Palliat Care. 2025. PMID: 39401339 Free PMC article.
-
Developing a comprehensive model of home-based long-term care for older people in Iran: a multi-method study.BMC Health Serv Res. 2025 Feb 22;25(1):298. doi: 10.1186/s12913-025-12434-0. BMC Health Serv Res. 2025. PMID: 39987070 Free PMC article.
-
Spread, participant experience, and implementation of Pallium Canada's Palliative Care ECHO project: a mixed methods study.BMC Palliat Care. 2025 Jul 1;24(1):176. doi: 10.1186/s12904-025-01804-4. BMC Palliat Care. 2025. PMID: 40598189 Free PMC article.
-
Potentially Inappropriate End of Life Care and Healthcare Costs in the Last 30 Days of Life in Regions Providing Integrated Palliative Care in the Netherlands: A Registration-based Study.Int J Integr Care. 2024 Jul 8;24(3):6. doi: 10.5334/ijic.7504. eCollection 2024 Jul-Sep. Int J Integr Care. 2024. PMID: 39005964 Free PMC article.
-
Association between Inappropriate End-of-Life Cancer Care and Specialist Palliative Care: A Retrospective Observational Study in Two Acute Care Hospitals.Cancers (Basel). 2024 Feb 8;16(4):721. doi: 10.3390/cancers16040721. Cancers (Basel). 2024. PMID: 38398112 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
