

TAVI in patients with low-flow low-gradient aortic stenosis-short-term and long-term outcomes
- PMID: 35320407
- PMCID: PMC9681695
- DOI: 10.1007/s00392-022-02011-4
TAVI in patients with low-flow low-gradient aortic stenosis-short-term and long-term outcomes
Abstract
Objectives: The study objective was to characterize different groups of low-flow low-gradient (LFLG) aortic stenosis (AS) and determine short-term outcomes and long-term mortality according to Valve Academic Research Consortium-3 (VARC-3) endpoint definitions.
Background: Characteristics and outcomes of patients with LFLG AS undergoing transcatheter aortic valve implantation (TAVI) are poorly understood.
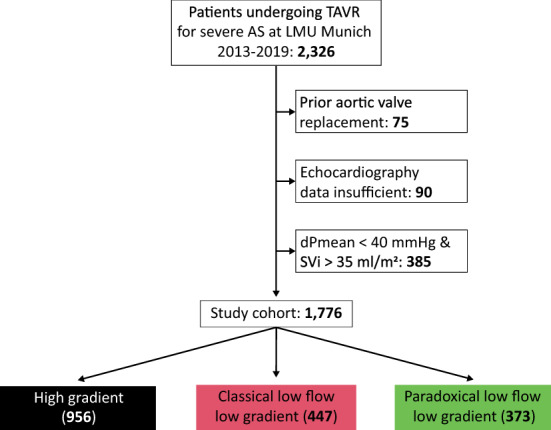
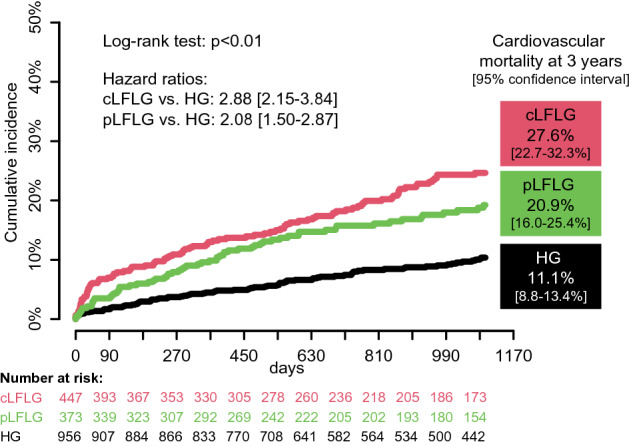
Methods: All patients undergoing TAVI at our center between 2013 and 2019 were screened. Patients were divided into three groups according to mean pressure gradient (dPmean), ejection fraction (LVEF), and stroke volume index (SVi): high gradient (HG) AS (dPmean ≥ 40 mmHg), classical LFLG (cLFLG) AS (dPmean < 40 mmHg, LVEF < 50%), and paradoxical LFLG (pLFLG) AS (dPmean < 40 mmHg, LVEF ≥ 50%, SVi ≤ 35 ml/m2).
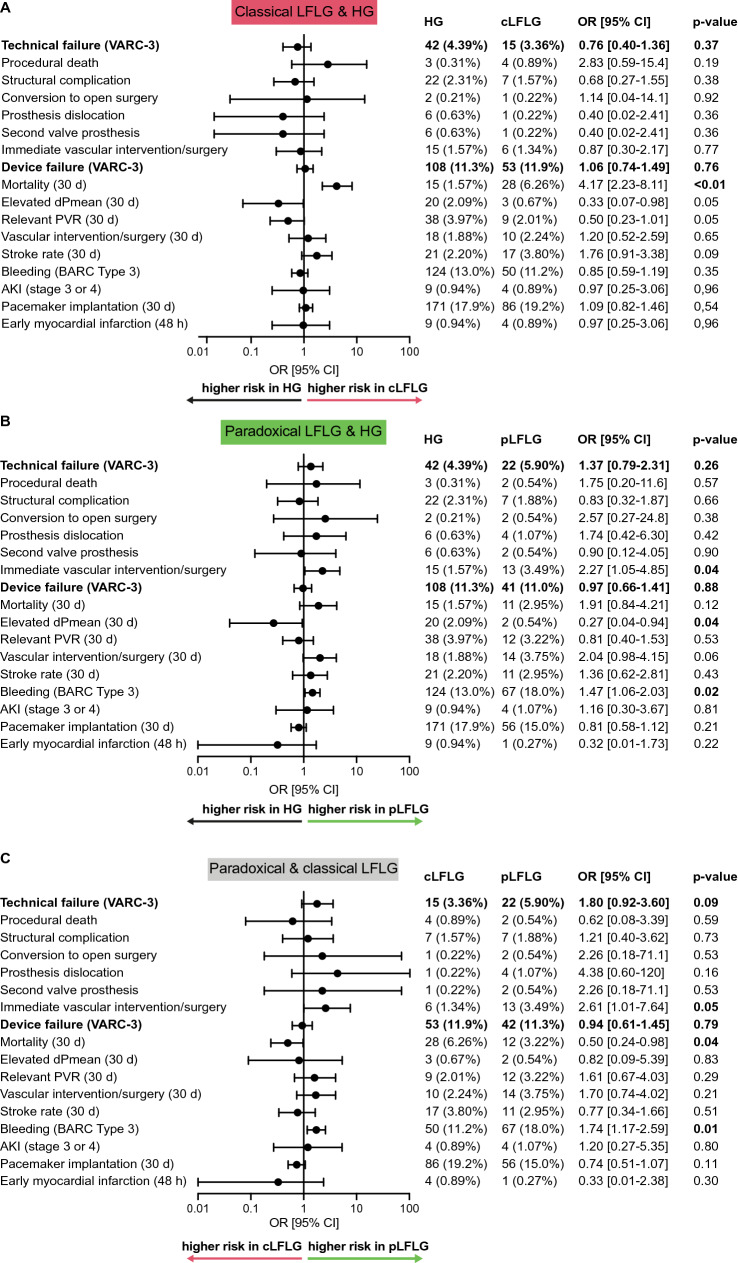
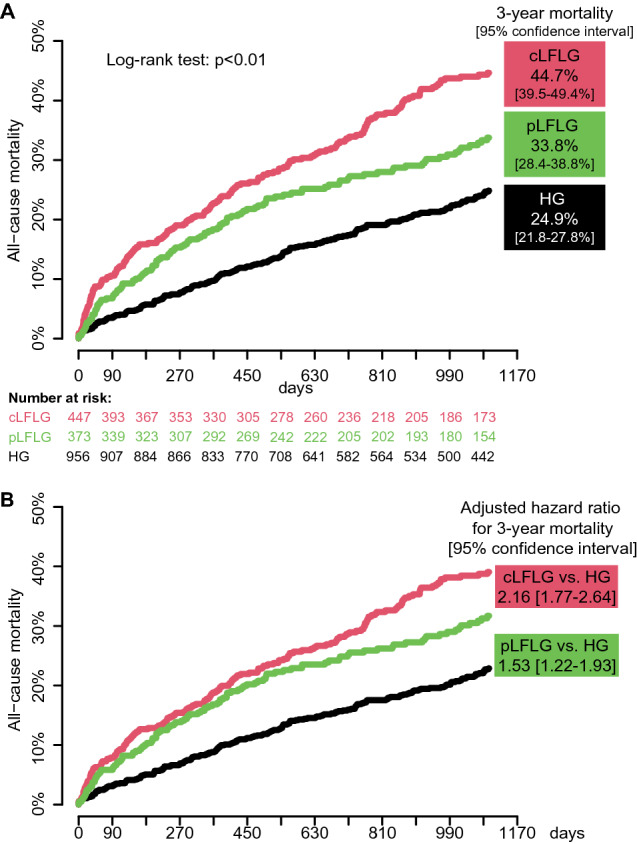
Results: We included 1776 patients (956 HG, 447 cLFLG, and 373 pLFLG patients). Most baseline characteristics differed significantly. Median Society of Thoracic Surgeons (STS) score was highest in cLFLG, followed by pLFLG and HG patients (5.0, 3.9 and 3.0, respectively, p < 0.01). Compared to HG patients, odds ratios for the short-term VARC-3 composite endpoints, technical failure (cLFLG, 0.76 [95% confidence interval, 0.40-1.36], pLFLG, 1.37 [0.79-2.31]) and device failure (cLFLG, 1.06 [0.74-1.49], pLFLG, 0.97 [0.66-1.41]) were similar, without relevant differences within LFLG patients. NYHA classes improved equally in all groups. Compared to HG, LFLG patients had a higher 3-year all-cause mortality (STS score-adjusted hazard ratios, cLFLG 2.16 [1.77-2.64], pLFLG 1.53 [1.22-193]), as well as cardiovascular mortality (cLFLG, 2.88 [2.15-3.84], pLFLG, 2.08 [1.50-2.87]).
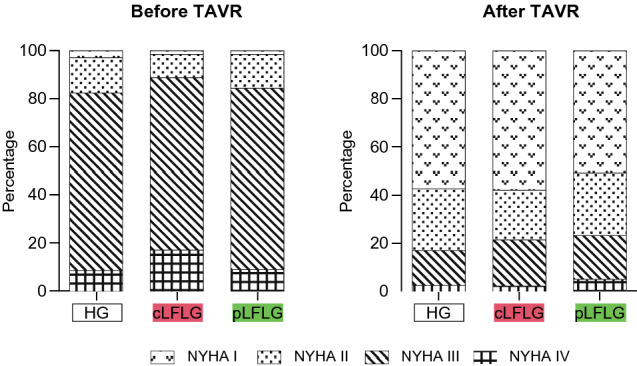
Conclusions: While 3-year mortality remains high after TAVI in LFLG compared to HG patients, symptoms improve in all subsets after TAVI.
Keywords: Aortic stenosis; Low-flow low-gradient; TAVI; VARC-3.
© 2022. The Author(s).
Conflict of interest statement
JS received speaker honoraria from AstraZeneca. DB received speaker honoraria from Abbott Vascular. MO received speaker honoraria and travel compensations from Abbott Medical, AstraZeneca, Abiomed, Bayer vital, BIOTRONIK, Bristol-Myers Squibb, CytoSorbents, Daiichi Sankyo Germany, Edwards Lifesciences Services, and Sedana Medical. JH received research support Abbott Vascular and Edwards Lifesciences. SD received speaker honoraria from AstraZeneca. All other authors report to have no conflicts of interests to declare.
Figures

References
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W, Neumann F-J, Myers P, Abdelhamid M, Achenbach S, Asteggiano R, Barili F, Borger MA, Carrel T, Collet J-P, Foldager D, Habib G, Hassager C, Irs A, Iung B, Jahangiri M, Katus HA, Koskinas KC, Massberg S, Mueller CE, Nielsen JC, Pibarot P, Rakisheva A, Roffi M, Rubboli A, Shlyakhto E, Siepe M, Sitges M, Sondergaard L, Sousa-Uva M, Tarantini G, Zamorano JL, Praz F, Milojevic M, Baldus S, Bauersachs J, Capodanno D, Conradi L, De Bonis M, De Paulis R, Delgado V, Freemantle N, Gilard M, Haugaa KH, Jeppsson A, Jüni P, Pierard L, Prendergast BD, Sádaba JR, Tribouilloy C, Wojakowski W. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2021 doi: 10.1093/eurheartj/ehab395. - DOI - PMC - PubMed
-
- Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ, Evolut Low Risk Trial I Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. 2019;380(18):1706–1715. doi: 10.1056/NEJMoa1816885. - DOI - PubMed
-
- Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR, Investigators P. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. 2019;380(18):1695–1705. doi: 10.1056/NEJMoa1814052. - DOI - PubMed
-
- Baumgartner HC, Hung JC-C, Bermejo J, Chambers JB, Edvardsen T, Goldstein S, Lancellotti P, LeFevre M, Miller F, Jr, Otto CM. Recommendations on the echocardiographic assessment of aortic valve stenosis: a focused update from the European association of cardiovascular imaging and the American society of echocardiography. Eur Heart J Cardiovasc Imaging. 2017;18(3):254–275. doi: 10.1093/ehjci/jew335. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
