

Posterior pelvic exenteration for ovarian cancer: surgical and oncological outcomes
- PMID: 35320883
- PMCID: PMC9024184
- DOI: 10.3802/jgo.2022.33.e31
Posterior pelvic exenteration for ovarian cancer: surgical and oncological outcomes
Abstract
Objective: Posterior pelvic exenteration (PPE) can be required to achieve complete resection in ovarian cancer (OC) patients with large pelvic disease. This study aimed to analyze morbidity, complete resection rate, and survival of PPE.
Methods: Ninety patients who underwent PPE in our Comprehensive Cancer Center between January 2010 and February 2021 were retrospectively identified. To analyze practice evolution, 2 periods were determined: P1 from 2010 to 2017 and P2 from 2018 to 2021.
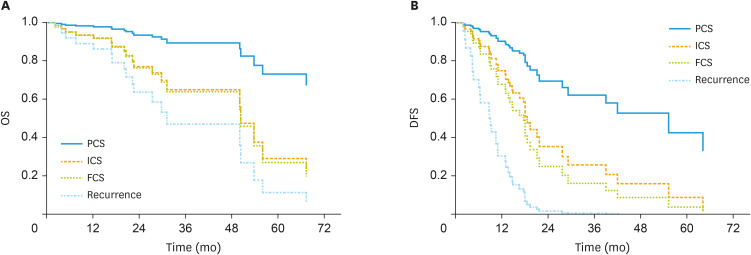
Results: A 82.2% complete resection rate after PPE was obtained, with rectal anastomosis in 96.7% of patients. Complication rate was at 30% (grade 3 in 9 patients), without significant difference according to periods or quality of resection. In a binary logistic regression adjusted on age and stoma, only age of 51-74 years old was associated with a lower rate of complication (odds ratio=0.223; p=0.026). Median overall and disease-free survivals (OS and DFS) from initial diagnosis were 75.21 and 29.84 months, respectively. A negative impact on OS and DFS was observed in case of incomplete resection, and on DFS in case of final cytoreductive surgery (FCS: after ≥6 chemotherapy cycles). Age ≥75-years had a negative impact on DFS for new OC surgery. For patients with complete resection, OS and DFS were decreased in case of interval cytoreductive surgery and FCS in comparison with primary cytoreductive surgery.
Conclusion: PPE is an effective surgical measure to achieve complete resection for a majority of patients. High rate of colorectal anastomosis was achieved without any mortality, with acceptable morbidity and high protective stoma rate.
Keywords: Ovarian Cancer; Pelvic Exenteration; Prognosis; Surgery; Survival.
Copyright © 2022. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology, and Japan Society of Gynecologic Oncology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Posterior pelvic exenteration, a crucial component in the surgeon's toolbox for optimizing surgical cytoreduction for advanced ovarian cancer.J Gynecol Oncol. 2022 May;33(3):e41. doi: 10.3802/jgo.2022.33.e41. Epub 2022 Feb 21. J Gynecol Oncol. 2022. PMID: 35320890 Free PMC article. No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Vergote I, Tropé CG, Amant F, Kristensen GB, Ehlen T, Johnson N, et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N Engl J Med. 2010;363:943–953. - PubMed
-
- Kehoe S, Hook J, Nankivell M, Jayson GC, Kitchener H, Lopes T, et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): an open-label, randomised, controlled, non-inferiority trial. Lancet. 2015;386:249–257. - PubMed
-
- Colombo N, Sessa C, du Bois A, Ledermann J, McCluggage WG, McNeish I, et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease†. Ann Oncol. 2019;30:672–705. - PubMed
