

Effect Modification of Hyperuricemia, Cardiovascular Risk, and Age on Chronic Kidney Disease in China: A Cross-Sectional Study Based on the China Health and Nutrition Survey Cohort
- PMID: 35321107
- PMCID: PMC8934943
- DOI: 10.3389/fcvm.2022.853917
Effect Modification of Hyperuricemia, Cardiovascular Risk, and Age on Chronic Kidney Disease in China: A Cross-Sectional Study Based on the China Health and Nutrition Survey Cohort
Abstract
Introduction: The question of whether the increased burden of chronic kidney disease (CKD) is caused by the interaction of hyperuricemia and cardiovascular disease (CVD) risk factors or is accelerated by aging remains unresolved. The purpose of this study is to better understand the effect modification of hyperuricemia, cardiovascular risk, and age on CKD among the Chinese population.
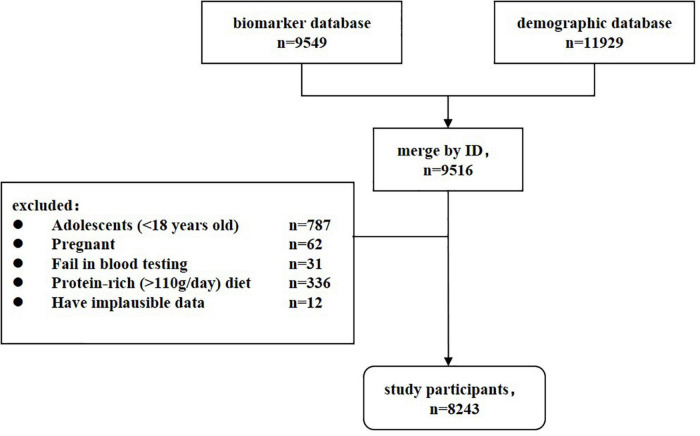
Methods: This cross-sectional study of 8243 participants was derived from the China Health and Nutrition Survey (CHNS) in 2009. Inclusion criteria included age ≥18 years, non-pregnancy, and no history of high-protein diet prior to blood test. Demographics, comorbidities, health-related behaviors, and serum biomarkers were collected. Interaction association of hyperuricemia, CVD risk and age with CKD were analyzed using Logistic regression.
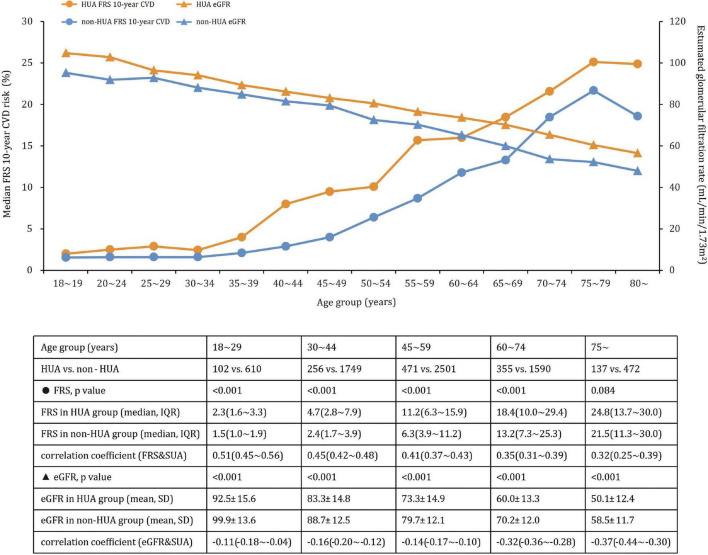
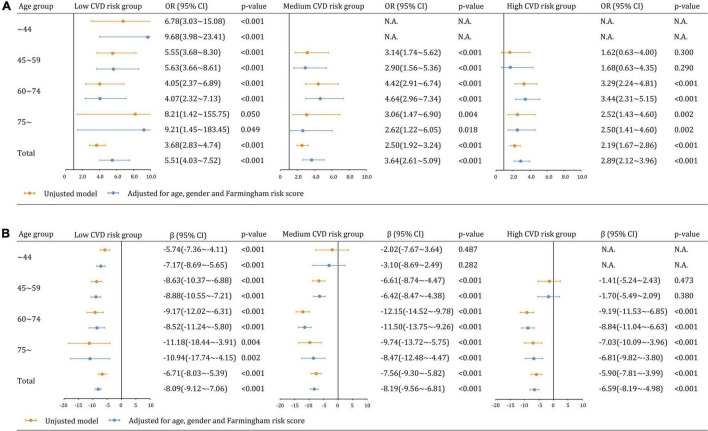
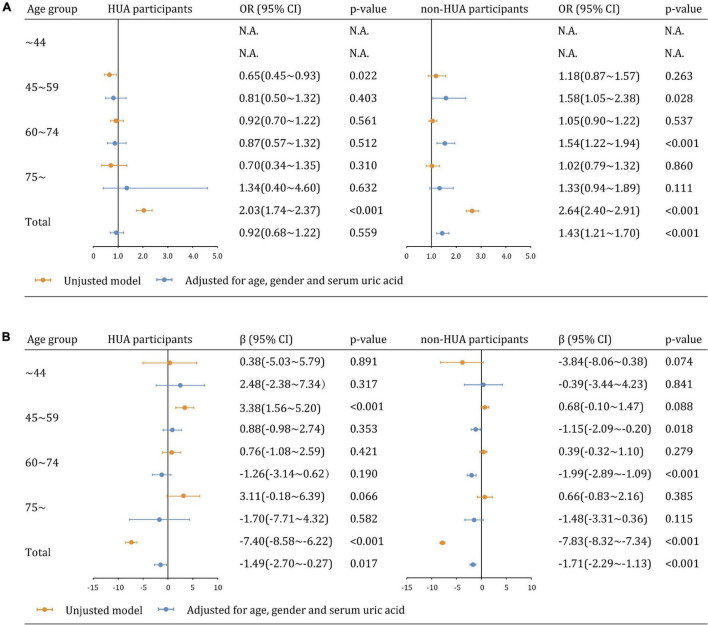
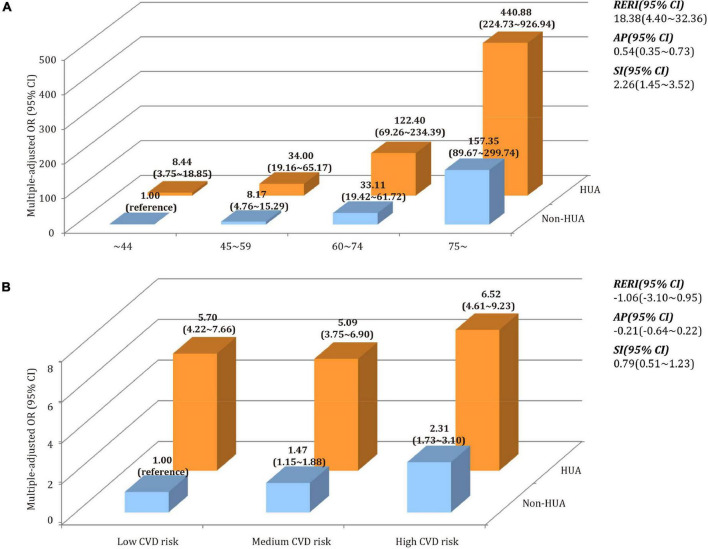
Results: CKD was detected in 359 (27.2%, 95% CI 24.8∼29.7%) of 1321 participants with hyperuricemia and 680 (9.8%, 95% CI 9.1∼10.5%) of 6,922 participants without hyperuricemia, and these patterns remained significant after controlling for age, gender, and Framingham risk score (adjusted odds ratio [aOR] 3.82, 95% CI 3.20∼4.57). We found a negative multiplicative interaction between hyperuricemia and CVD risk on CKD. The aOR in low-CVD risk groups was 5.51 (95% CI 4.03∼7.52), followed by medium-CVD risk groups (aOR: 3.64, 95% CI 2.61∼5.09) and high-CVD risk groups (aOR: 2.89, 95% CI 2.12∼3.96). CVD risk was less associated with CKD in hyperuricemia group (aOR: 0.92, 95% CI 0.68∼1.22) than in non-hyperuricemia group (aOR: 1.43, 95% CI 1.21∼1.70). Furthermore, hyperuricemia and age had a significant additive effect on CKD, with a synergy index of 2.26 (95% CI 1.45∼3.52). Coexisting with older age and hyperuricemia, the likelihood of developing CKD was higher than the sum of the two alone.
Conclusion: The link between hyperuricemia and CKD begins at a young age and becomes stronger in the low CVD risk group. For young adults, early detection of hyperuricemia, routine CVD risk assessment, and timely intervention of modifiable factors are warranted.
Keywords: China health and nutrition survey; cardiovascular disease risk; chronic kidney disease; hyperuricemia; interaction analysis.
Copyright © 2022 Li, Zhu, Xie, Jin, Zhou, Fang and Ding.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Association of chronic kidney disease and cardiovascular disease risk with all-cause mortality: an interaction, joint and mediation analysis in Chinese adults.BMC Public Health. 2025 May 7;25(1):1685. doi: 10.1186/s12889-025-22924-9. BMC Public Health. 2025. PMID: 40335982 Free PMC article.
-
Hyperuricemia and its association with adiposity and dyslipidemia in Northwest China: results from cardiovascular risk survey in Xinjiang (CRS 2008-2012).Lipids Health Dis. 2020 Apr 1;19(1):58. doi: 10.1186/s12944-020-01211-z. Lipids Health Dis. 2020. PMID: 32238146 Free PMC article.
-
The prevalence of diabetes mellitus with chronic kidney disease in adults and associated factors in Songjiang District, Shanghai.Ann Palliat Med. 2021 Jul;10(7):7214-7224. doi: 10.21037/apm-21-803. Epub 2021 Jun 29. Ann Palliat Med. 2021. PMID: 34263637
-
Should eGFR and albuminuria be added to the Framingham risk score? Chronic kidney disease and cardiovascular disease risk prediction.Nephron Clin Pract. 2011;119(2):c171-7; discussion c177-8. doi: 10.1159/000325669. Epub 2011 Jul 28. Nephron Clin Pract. 2011. PMID: 21811078 Review.
-
Clinical epidemiology of cardiovascular disease in chronic kidney disease prior to dialysis.Semin Dial. 2003 Mar-Apr;16(2):101-5. doi: 10.1046/j.1525-139x.2003.16025.x. Semin Dial. 2003. PMID: 12641872 Review.
Cited by
-
Cost-effectiveness of universal genetic screening for familial hypercholesterolemia in young adults aged 18-40 years in China.BMC Med. 2025 Mar 5;23(1):139. doi: 10.1186/s12916-025-03966-7. BMC Med. 2025. PMID: 40045404 Free PMC article.
-
Higher dietary acid load is associated with hyperuricemia in Chinese adults: a case-control study.BMC Endocr Disord. 2022 Nov 18;22(1):286. doi: 10.1186/s12902-022-01192-3. BMC Endocr Disord. 2022. PMID: 36401201 Free PMC article.
-
Associations of specific types of physical activities with 10-year risk of cardiovascular disease among adults: Data from the national health and nutrition examination survey 1999-2006.Front Public Health. 2022 Jul 25;10:964862. doi: 10.3389/fpubh.2022.964862. eCollection 2022. Front Public Health. 2022. PMID: 35958867 Free PMC article.
-
Temporal trends in prevalence and mortality for chronic kidney disease in China from 1990 to 2019: an analysis of the Global Burden of Disease Study 2019.Clin Kidney J. 2022 Oct 10;16(2):312-321. doi: 10.1093/ckj/sfac218. eCollection 2023 Feb. Clin Kidney J. 2022. PMID: 36755850 Free PMC article.
-
Machine learning-based prediction models for renal impairment in Chinese adults with hyperuricaemia: risk factor analysis.Sci Rep. 2025 Mar 15;15(1):8968. doi: 10.1038/s41598-025-88632-x. Sci Rep. 2025. PMID: 40089508 Free PMC article.
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Levin A, Stevens P, Bilous RW, Coresh J, Francisco A, Jong PE, et al. Kidney disease: improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. (2013) 3:1–150. 10.1038/kisup.2012.73 - DOI
-
- Liu M, Li XC, Lu L, Cao Y, Sun RR, Chen S, et al. Cardiovascular disease and its relationship with chronic kidney disease. Eur Rev Med Pharmacol Sci. (2014) 18:2918–26. - PubMed
LinkOut - more resources
Full Text Sources