

Does the Efficacy of Behavior Management Techniques Differ Between Children From Single-Child and Multi-Child Families?: A Quasi-Experimental Study
- PMID: 35321197
- PMCID: PMC8936677
- DOI: 10.3389/fpubh.2022.840483
Does the Efficacy of Behavior Management Techniques Differ Between Children From Single-Child and Multi-Child Families?: A Quasi-Experimental Study
Abstract
Aim: Behavior management techniques (BMTs) efficiently deliver dental treatment to children with dental anxiety. The objective of this quasi-experimental study was to examine whether the efficacy of BMTs applied for the improvement of compliance in pediatric patients differs between children 3-10-year-olds from single-child and multi-child families.
Materials and methods: In this quasi-experimental, 197 caregiver-child couples were divided into two groups: single-child group (116 couples) and multi-child group (81 couples). Children's pre- and post-treatment anxiety levels were measured by facial mood scale (FMS) and Frankl Behavior Rating Scale (FBRS), respectively.Caregivers' dental anxiety was measured by the Chinese version of the Modified Dental Anxiety Scale (MDAS), which was included in the self-designed questionnaire. Data were analyzed by using the Mann-Whitney U-test, chi-square tests, and binary multivariate regression analysis.
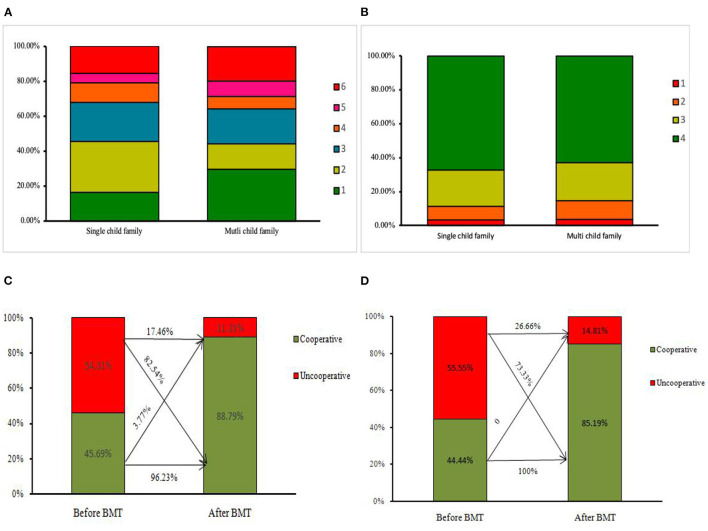
Results: There was no statistically significant difference in the demographic characteristics of the children between the two groups. BMTs were found to be capable of reducing children's dental anxiety (CDA): the compliance rate was 45.69-88.79% in the single-child group and 44.44-85.79% in the multi-child group pre- and post-BMTs, but there was no significant difference in the change of compliance between the two groups (p > 0.05). In the subgroup analysis, parenting style (odds ratio [OR] = 0.054, p < 0.05) and father's education (OR = 8.19, p < 0.05) affected the varies of children's compliance in the single-child group. In contrast, in the multi-child group, gender (OR = 8.004, p < 0.05) and mother's occupation (OR = 0.017, p < 0.05) were associated with these changes in compliance.
Conclusions: In this study, BMTs were proved to be beneficial in improving compliance in 3- to 10-year-olds children in dental treatment. Though there was no significant difference in the change of compliance between children from single-child and multi-child families, different associated factors may affect the two groups. Therefore, the related family factors should be taken into account when professionals manage each child's behavior in dental practice.
Keywords: behavior management techniques; children's dental anxiety; compliance; multi-child; single-child.
Copyright © 2022 Dai, Wu, Hu, Li and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The Influence of Parenting Style and Child Temperament on Child-Parent-Dentist Interactions.Pediatr Dent. 2015 Jul-Aug;37(4):342-7. Pediatr Dent. 2015. PMID: 26314601
-
Can birth order affect temperament, anxiety and behavior in 5 to 7-year-old children in the dental setting?J Contemp Dent Pract. 2011 Jul 1;12(4):225-31. doi: 10.5005/jp-journals-10024-1039. J Contemp Dent Pract. 2011. PMID: 22186855 Clinical Trial.
-
The impact of maternal emotional intelligence and parenting style on child anxiety and behavior in the dental setting.Med Oral Patol Oral Cir Bucal. 2012 Nov 1;17(6):e1089-95. doi: 10.4317/medoral.17839. Med Oral Patol Oral Cir Bucal. 2012. PMID: 22926462 Free PMC article.
-
[Simple obesity in children. A study on the role of nutritional factors].Med Wieku Rozwoj. 2006 Jan-Mar;10(1):3-191. Med Wieku Rozwoj. 2006. PMID: 16733288 Review. Polish.
-
The Influence of Parenting Style on Child Behavior and Dental Anxiety.Pediatr Dent. 2018 Sep 15;40(5):327-333. Pediatr Dent. 2018. PMID: 30355427
References
-
- Chhabra N, Chhabra A, Walia G. Prevalence of dental anxiety and fear among five to ten year old children: a behaviour based cross sectional study. Minerva Stomatol. (2012) 61:83–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous