

Fetal Pain in the First Trimester
- PMID: 35321491
- PMCID: PMC8935428
- DOI: 10.1177/00243639211059245
Fetal Pain in the First Trimester
Abstract
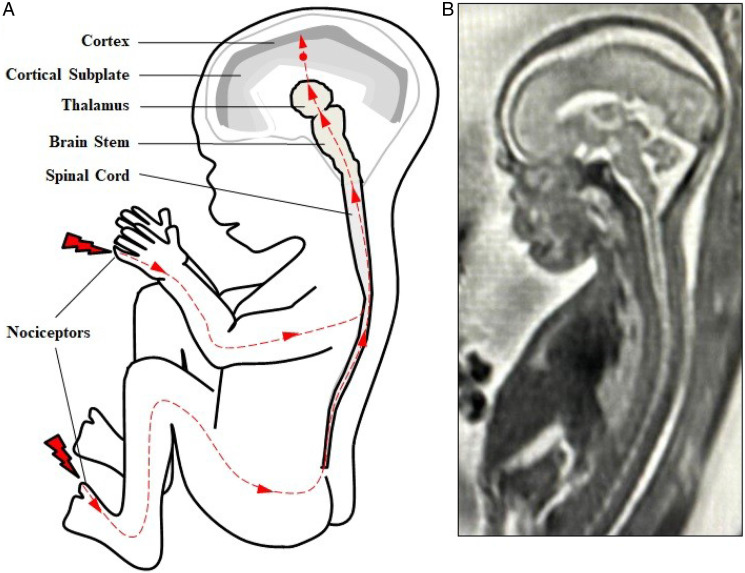
Fetal pain perception has important implications for fetal surgery, as well as for abortion. Current neuroscientific evidence indicates the possibility of fetal pain perception during the first trimester (<14 weeks gestation). Evidence for this conclusion is based on the following findings: (1) the neural pathways for pain perception via the cortical subplate are present as early as 12 weeks gestation, and via the thalamus as early as 7-8 weeks gestation; (2) the cortex is not necessary for pain to be experienced; (3) consciousness is mediated by subcortical structures, such as the thalamus and brainstem, which begin to develop during the first trimester; (4) the neurochemicals in utero do not cause fetal unconsciousness; and (5) the use of fetal analgesia suppresses the hormonal, physiologic, and behavioral responses to pain, avoiding the potential for both short- and long-term sequelae. As the medical evidence has shifted in acknowledging fetal pain perception prior to viability, there has been a gradual change in the fetal pain debate, from disputing the existence of fetal pain to debating the significance of fetal pain. The presence of fetal pain creates tension in the practice of medicine with respect to beneficence and nonmaleficence.
Keywords: fetal analgesia; fetal anesthesia; fetal awareness; fetal nociception; fetal pain.
© Catholic Medical Association 2021.
Conflict of interest statement
Declaration of Conflicting Interest: The author(s) declared that there is no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
