

PARP inhibitors chemopotentiate and synergize with cisplatin to inhibit bladder cancer cell survival and tumor growth
- PMID: 35321693
- PMCID: PMC8944004
- DOI: 10.1186/s12885-022-09376-9
PARP inhibitors chemopotentiate and synergize with cisplatin to inhibit bladder cancer cell survival and tumor growth
Abstract
Background: Management of bladder cancer (BLCA) has not changed significantly in the past few decades, with platinum agent chemotherapy being used in most cases. Chemotherapy reduces tumor recurrence after resection, but debilitating toxicities render a large percentage of patients ineligible. Recently approved immunotherapy can improve outcomes in only a third of metastatic BLCA patients. Therefore, more options for therapy are needed. In this study, we explored the efficacy of PARP inhibitors (PARPi) as single agents or as combinations with platinum therapy.
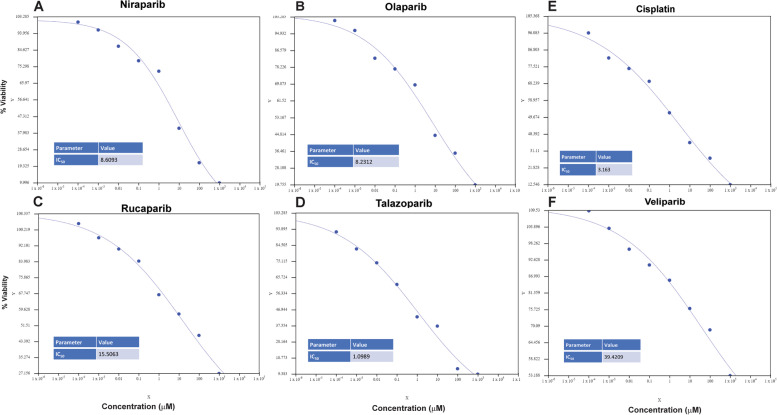
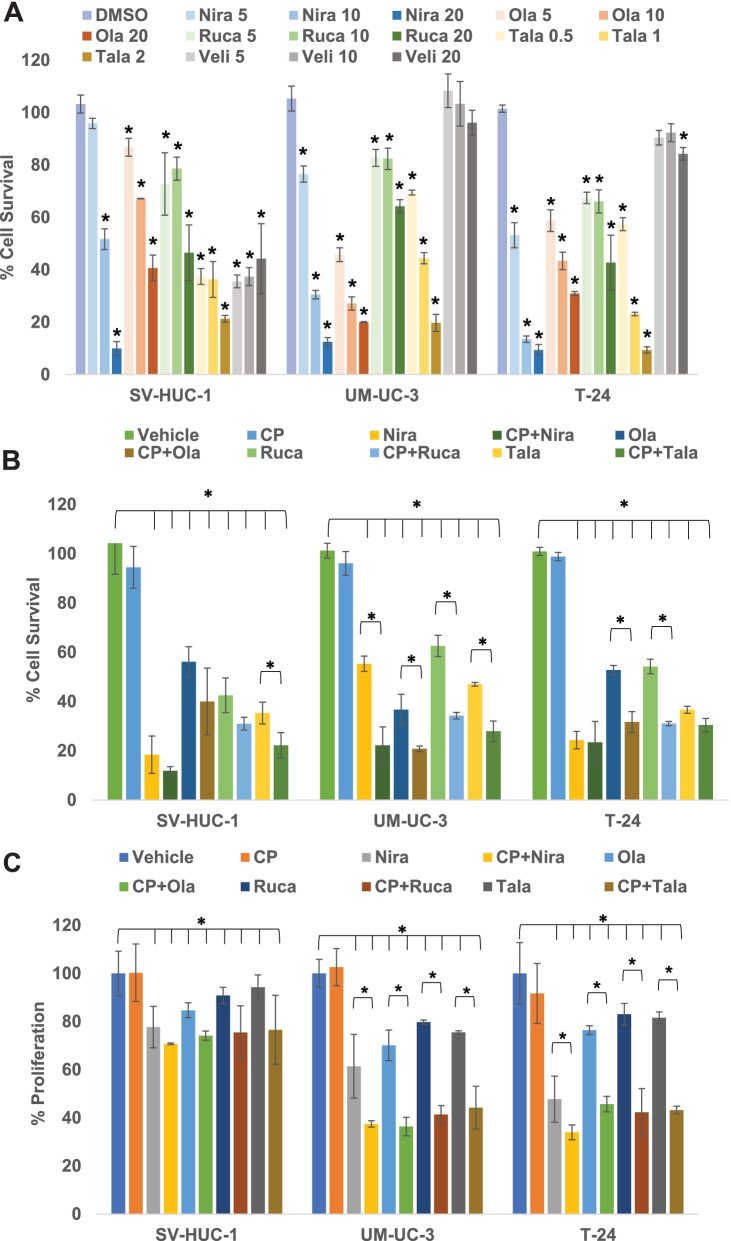
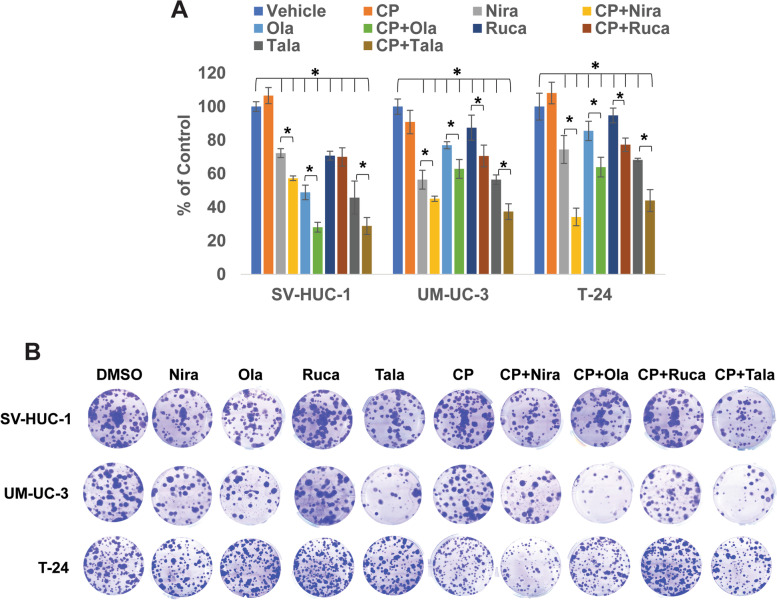
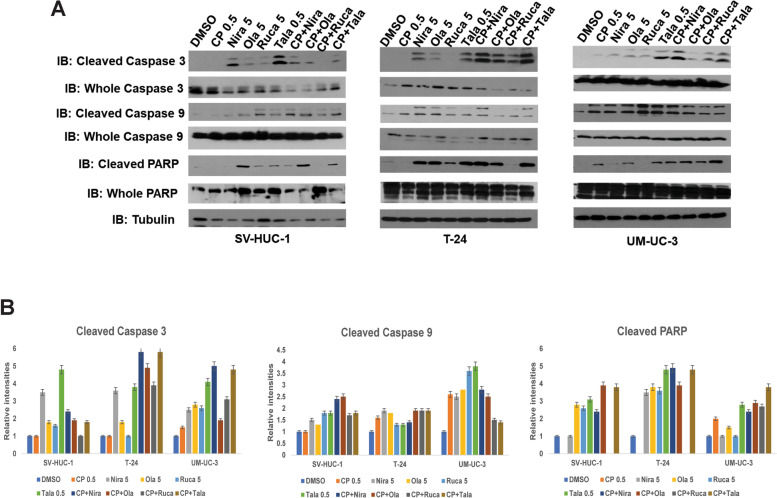
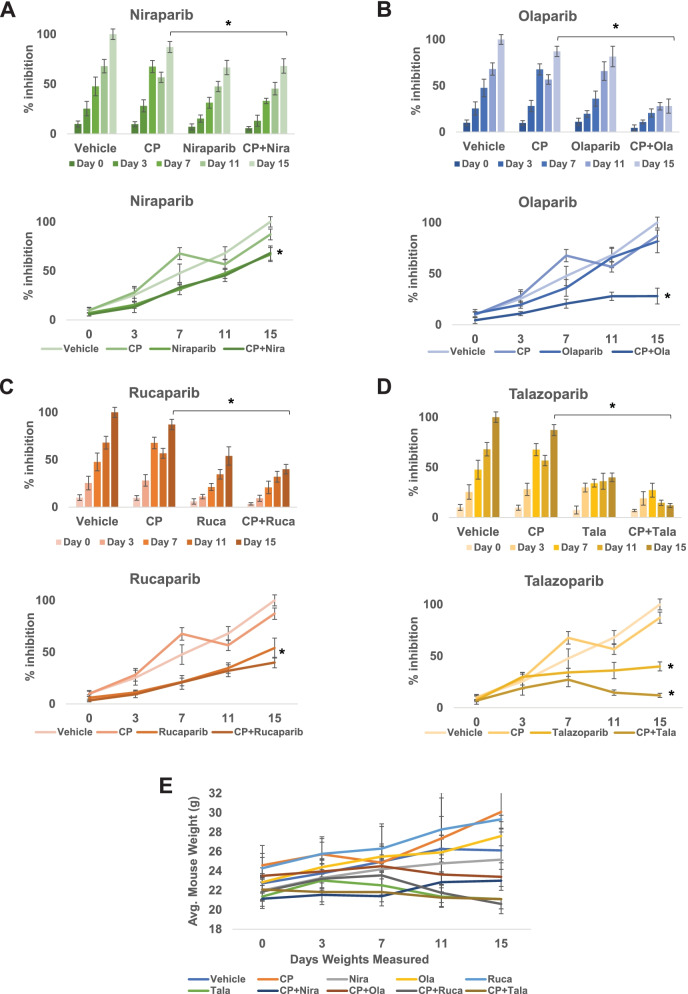
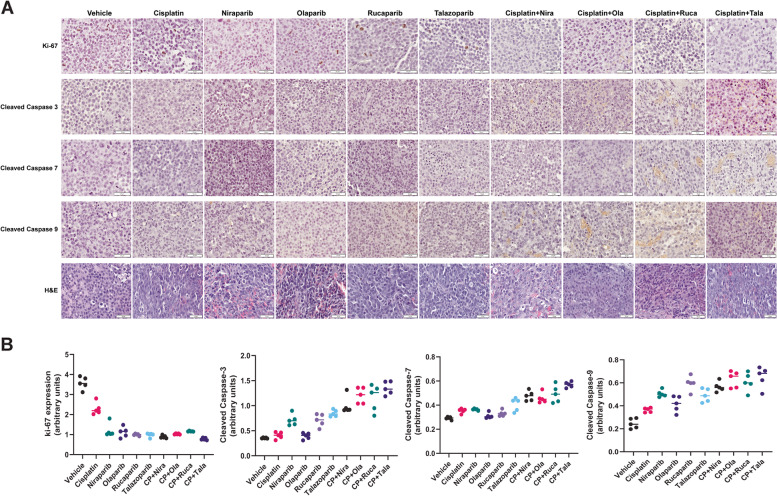
Methods: We treated BLCA cells with PARPi (olaparib, niraparib, rucaparib, veliparib, or talazoparib) alone or as the combination of cisplatin with PARPi. We then measured their survival, proliferation, apoptosis, as well as their ability to form colonies. BLCA xenografts in male SCID mice were treated similarly, followed by the assessment of their growth, proliferation, and apoptosis.
Results: PARPi niraparib and talazoparib were effective in reducing BLCA cell survival as single agents. Combinations of Cisplatin with talazoparib and niraparib effectively reduced the survival of BLCA cells, while veliparib was not effective even at high concentrations. In vivo, the combinations of cisplatin with niraparib, rucaparib, or talazoparib reduced BLCA xenograft growth significantly.
Conclusions: We provide evidence that PARPi can be effective against BLCA as single agents or as combinatorial therapy with cisplatin.
Keywords: Bladder cancer; Cisplatin; Combination therapy; DNA damage repair; PARP inhibition; Urothelial carcinoma.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no relevant competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
