

State-of-the-art review of lung imaging in cystic fibrosis with recommendations for pulmonologists and radiologists from the "iMAging managEment of cySTic fibROsis" (MAESTRO) consortium
- PMID: 35321929
- PMCID: PMC9489084
- DOI: 10.1183/16000617.0173-2021
State-of-the-art review of lung imaging in cystic fibrosis with recommendations for pulmonologists and radiologists from the "iMAging managEment of cySTic fibROsis" (MAESTRO) consortium
Abstract
Objective: Imaging represents an important noninvasive means to assess cystic fibrosis (CF) lung disease, which remains the main cause of morbidity and mortality in CF patients. While the development of new imaging techniques has revolutionised clinical practice, advances have posed diagnostic and monitoring challenges. The authors aim to summarise these challenges and make evidence-based recommendations regarding imaging assessment for both clinicians and radiologists.
Study design: A committee of 21 experts in CF from the 10 largest specialist centres in Italy was convened, including a radiologist and a pulmonologist from each centre, with the overall aim of developing clear and actionable recommendations for lung imaging in CF. An a priori threshold of at least 80% of the votes was required for acceptance of each statement of recommendation.
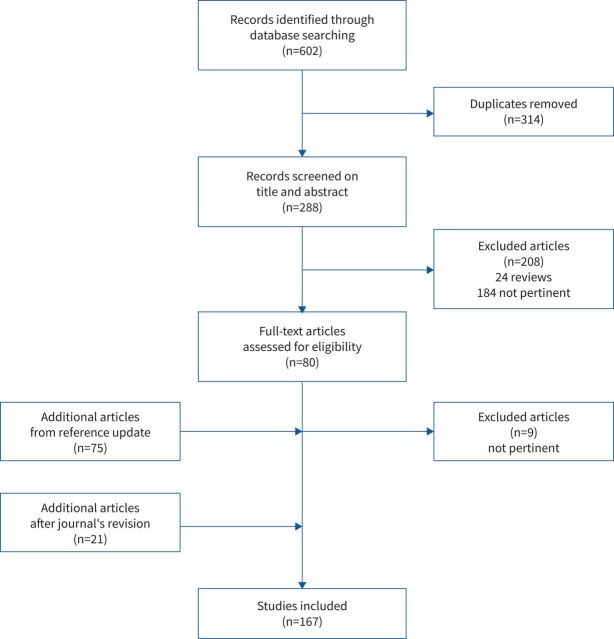
Results: After a systematic review of the relevant literature, the committee convened to evaluate 167 articles. Following five RAND conferences, consensus statements were developed by an executive subcommittee. The entire consensus committee voted and approved 28 main statements.
Conclusions: There is a need for international guidelines regarding the appropriate timing and selection of imaging modality for patients with CF lung disease; timing and selection depends upon the clinical scenario, the patient's age, lung function and type of treatment. Despite its ubiquity, the use of the chest radiograph remains controversial. Both computed tomography and magnetic resonance imaging should be routinely used to monitor CF lung disease. Future studies should focus on imaging protocol harmonisation both for computed tomography and for magnetic resonance imaging. The introduction of artificial intelligence imaging analysis may further revolutionise clinical practice by providing fast and reliable quantitative outcomes to assess disease status. To date, there is no evidence supporting the use of lung ultrasound to monitor CF lung disease.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: P. Ciet reports personal fees from Editamed, during the conduct of the study. S. Bertolo reports personal fees from Vertex pharmaceuticals, outside the submitted work. M. Ros reports personal fees from Vertex Pharmaceuticals, personal fees from Chiesi Farmaceutici, outside the submitted work. R. Casciaro has nothing to disclose. M. Cipolli has nothing to disclose. S. Colagrande reports that during the last 5 years, he has had and has various projects in place that have involved remuneration, which has always been devolved to the SBSC department for which Prof. Colagrande works. This refers to experimental/conventional activities for which it has received compensation. Nothing has ever been personally perceived by Prof. Colagrande and all the part destined to the university was conferred to the department. The companies involved were Novartis, Sanofi, Lilly, Celther, Pfizer, Janssen, etc. All the fees have been paid following the signing of a contract among the company, the university and the Hospital. S. Costa has nothing to disclose. V. Galici has nothing to disclose. A. Gramegna has nothing to disclose. C. Lanza has nothing to disclose. F. Lucca has nothing to disclose. L. Macconi has nothing to disclose. F. Majo has nothing to disclose. A. Paciaroni has nothing to disclose. G.F. Parisi has nothing to disclose. F. Rizzo has nothing to disclose. I. Salamone has nothing to disclose. T. Santangelo has nothing to disclose. L. Scudeller has nothing to disclose. L. Saba has nothing to disclose. P. Tomà has nothing to disclose. G. Morana has nothing to disclose.
References
-
- Cystic Fibrosis Foundation . Patient Registry Annual Data Report. 2020. Available from: www.cff.org/sites/default/files/2021-10/2019-Patient-Registry-Annual-Dat...