

Reconstructing antibody dynamics to estimate the risk of influenza virus infection
- PMID: 35322048
- PMCID: PMC8943152
- DOI: 10.1038/s41467-022-29310-8
Reconstructing antibody dynamics to estimate the risk of influenza virus infection
Erratum in
-
Author Correction: Reconstructing antibody dynamics to estimate the risk of influenza virus infection.Nat Commun. 2023 Feb 23;14(1):1032. doi: 10.1038/s41467-023-36822-4. Nat Commun. 2023. PMID: 36823190 Free PMC article. No abstract available.
Abstract
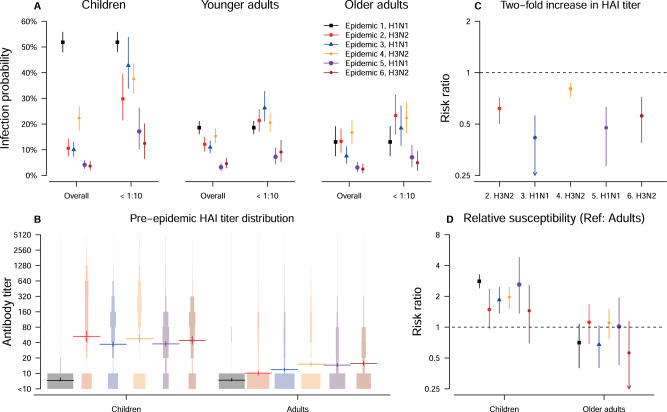
For >70 years, a 4-fold or greater rise in antibody titer has been used to confirm influenza virus infections in paired sera, despite recognition that this heuristic can lack sensitivity. Here we analyze with a novel Bayesian model a large cohort of 2353 individuals followed for up to 5 years in Hong Kong to characterize influenza antibody dynamics and develop an algorithm to improve the identification of influenza virus infections. After infection, we estimate that hemagglutination-inhibiting (HAI) titers were boosted by 16-fold on average and subsequently decrease by 14% per year. In six epidemics, the infection risks for adults were 3%-19% while the infection risks for children were 1.6-4.4 times higher than that of younger adults. Every two-fold increase in pre-epidemic HAI titer was associated with 19%-58% protection against infection. Our inferential framework clarifies the contributions of age and pre-epidemic HAI titers to characterize individual infection risk.
© 2022. The Author(s).
Conflict of interest statement
B.J.C. consults for AstraZeneca, Fosun Pharma, GlaxoSmithKline, Moderna, Pfizer, Roche and Sanofi Pasteur. The authors report no other potential competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
