

Comparison of soft tissue simulations between two planning software programs for orthognathic surgery
- PMID: 35322115
- PMCID: PMC8943157
- DOI: 10.1038/s41598-022-08991-7
Comparison of soft tissue simulations between two planning software programs for orthognathic surgery
Abstract
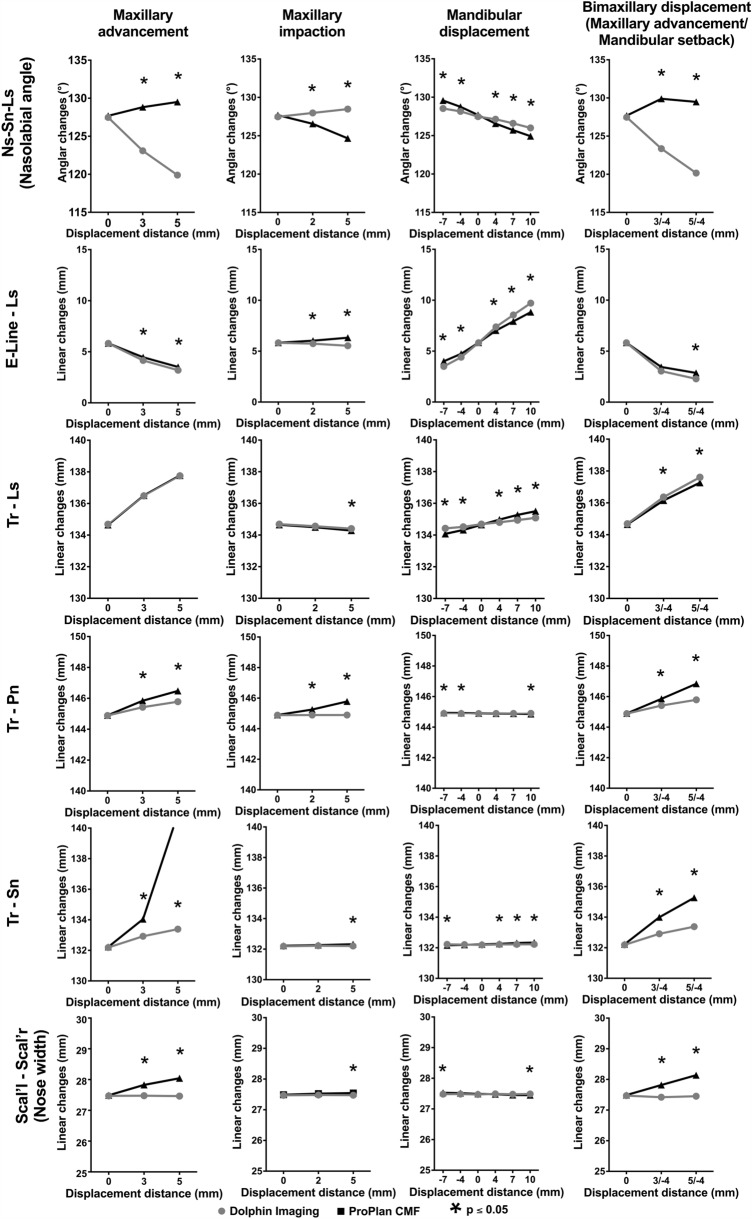
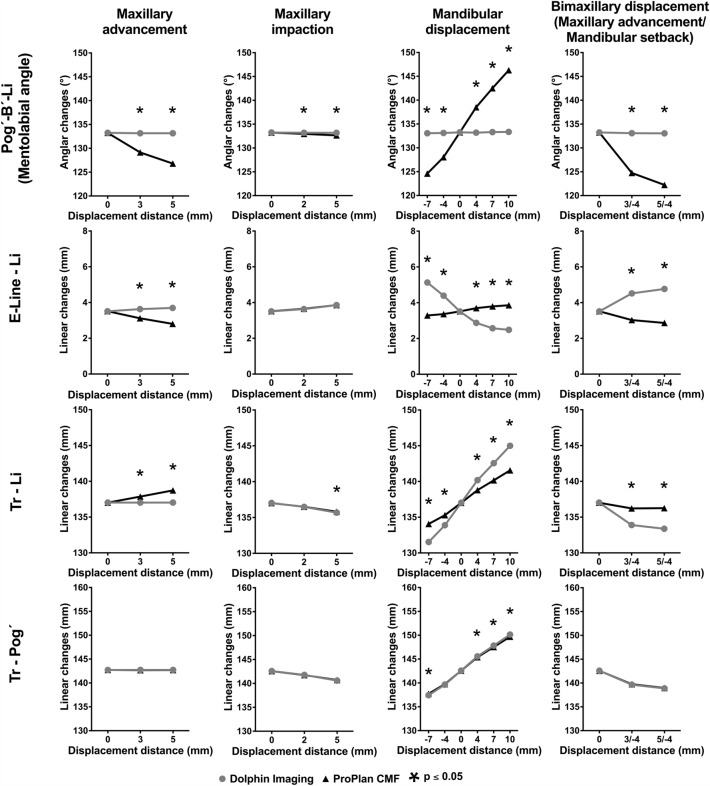
The aim of this study was to compare the soft tissue predicative abilities of two established programs depending on the surgical technique and amount of displacement. On the basis of 50 computed tomography images, 11 orthognathic operations with differences in displacement distances and technique (maxillary advancement, MxA; maxillary impaction, MxI; mandibular setback, MnS; mandibular advancement, MnA bimaxillary displacement, MxA/MnS) as well as corresponding soft tissue predictions were simulated using the programs Dolphin (D) and ProPlan (PP). For all the soft tissue predictions by the two programs, eight linear and two angular measurements were performed and compared. The simulation of maxillary impaction showed a similar soft tissue behaviour between the two programs. However, differences or divergent behaviours were observed for other procedures. In the middle third of the face these significant differences concerned in particular the nasolabial angle (Ns-Sn-Ls)(5 mm-MA, D: 119.9 ± 8.6° vs. PP: 129.5 ± 8.4°; 7 mm-MnS: D: 128.5 ± 8.2° vs. PP: 129.6 ± 8.1°; 10 mm-MnA D: 126.0 ± 8.0° vs. PP: 124.9 ± 8.4°; 5 mm-MxA/4 mm-MnS, D: 120.2 ± 8.7° vs. PP: 129.9 ± 8.3°; all p < 0.001) and in the lower third the mentolabial angle (Pog´-B´-Li) (5 mm-MA, D: 133.2 ± 11.4° vs. PP: 126.8 ± 11.6°; 7 mm-MnS: D: 133.1 ± 11.3° vs. PP: 124.6 ± 11.9°; 10 mm-MnA D: 133.3 ± 11.5° vs. PP: 146.3 ± 11.1°; bignathic 5 mm-MxA/4 mm-MnS, D: 133.1 ± 11.4° vs. PP: 122.7 ± 11.9°; all p < 0.001) and the distance of the inferior lip to the aesthetic Line (E-Line-Li) (5 mm-MA, D: 3.7 ± 2.3 mm vs. PP: 2.8 ± 2.5 mm; 7 mm-MnS: D: 5.1 ± 3.0 mm vs. PP: 3.3 ± 2.3 mm; 10 mm-MnA D: 2.5 ± 1.6 mm vs. PP: 3.9 ± 2.8 mm; bignathic 5 mm-MxA/4 mm-MnS, D: 4.8 ± 3.0 mm vs. PP: 2.9 ± 2.0 mm; all p < 0.001). The soft tissue predictions by the tested programs differed in simulation outcome, which led to the different, even divergent, results. However, the significant differences are often below a clinically relevant level. Consequently, soft tissue prediction must be viewed critically, and its actual benefit must be clarified.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Aboul-Hosn Centenero, S. & Hernandez-Alfaro, F. 3D planning in orthognathic surgery: CAD/CAM surgical splints and prediction of the soft and hard tissues results - our experience in 16 cases. J. Craniomaxillofac. Surg.40, 162–168. 10.1016/j.jcms.2011.03.014 (2012). - PubMed
-
- Mazzoni S, Bianchi A, Schiariti G, Badiali G, Marchetti C. Computer-aided design and computer-aided manufacturing cutting guides and customized titanium plates are useful in upper maxilla waferless repositioning. J. Oral Maxillofac. Surg. 2015;73:701–707. doi: 10.1016/j.joms.2014.10.028. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
