

Association of children wheezing diseases with meteorological and environmental factors in Suzhou, China
- PMID: 35322129
- PMCID: PMC8943037
- DOI: 10.1038/s41598-022-08985-5
Association of children wheezing diseases with meteorological and environmental factors in Suzhou, China
Abstract
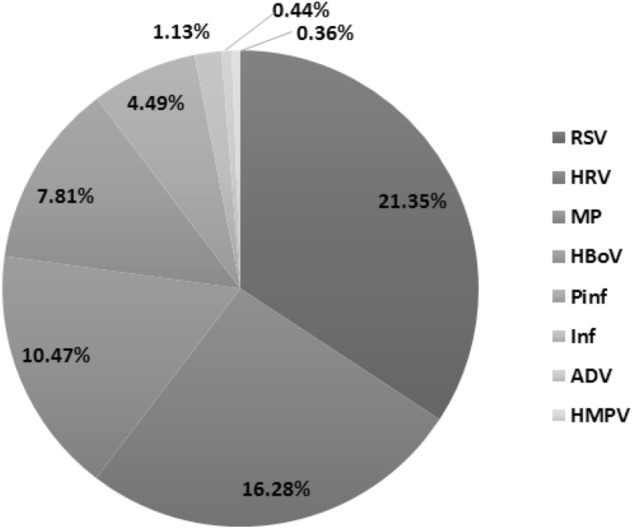
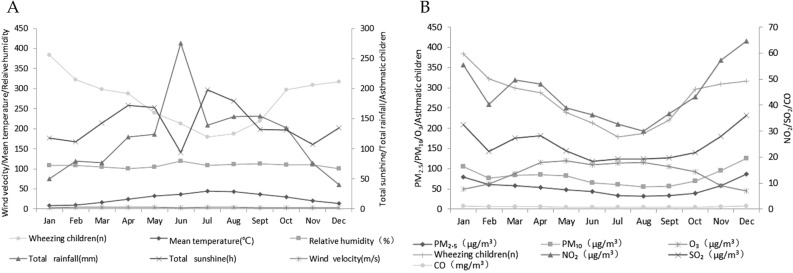
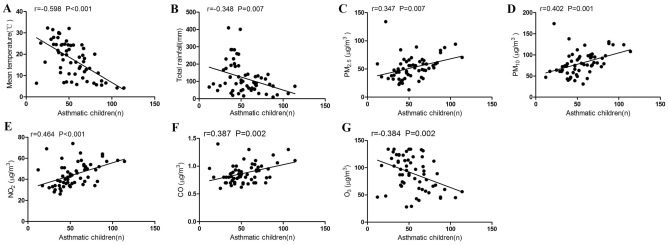
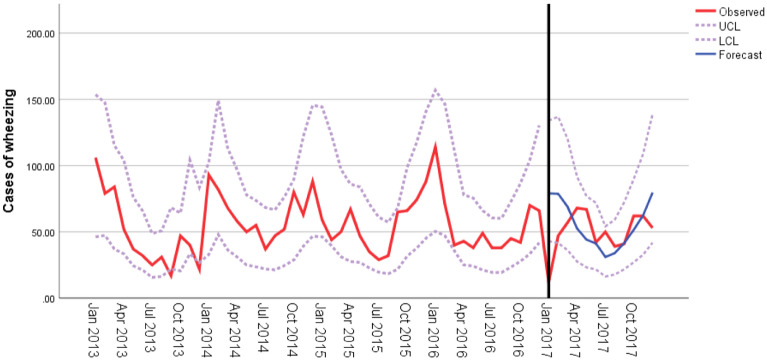
Wheezing diseases are one of the major chronic respiratory diseases in children. To explore the effects of meteorological and environmental factors on the prevalence of children wheezing diseases, clinical data of children hospitalized with wheezing diseases in Suzhou, China from 2013 to 2017 were collected. Meteorological and environmental factors from 2013 to 2017 were obtained from the local Meteorological Bureau and Environmental Protection Bureau. Relationships between wheezing diseases and meteorological and environmental factors were evaluated using Pearson's correlation and multivariate regression analysis. An autoregressive integrated moving average (ARIMA) model was used to estimate the effects of meteorological and environmental variables on children wheezing diseases. Children wheezing diseases were frequently presented in infants less than 12 months old (1897/2655, 58.28%), and the hospitalization rate was highest in winter (1024/3255, 31.46%). In pathogen-positive specimens, the top three pathogens were respiratory syncytial virus (21.35%), human rhinovirus (16.28%) and mycoplasma pneumoniae (10.47%). The seasonality of wheezing children number showed a distinctive winter peak. Children wheezing diseases were negatively correlated with average temperature (P < 0.001, r = - 0.598). The ARIMA (1,0,0)(0,0,0)12 model could be used to predict temperature changes associated wheezing diseases. Meteorological and environmental factors were associated with the number of hospitalized children with wheezing diseases and can be used as early warning indicators for the occurrence of wheezing diseases and prevalence of virus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Prevalence of rhinovirus in wheezing children: a comparison with respiratory syncytial virus wheezing.Braz J Infect Dis. 2016 Mar-Apr;20(2):179-83. doi: 10.1016/j.bjid.2015.12.005. Epub 2016 Feb 7. Braz J Infect Dis. 2016. PMID: 26859065 Free PMC article.
-
Association of meteorological factors with childhood viral acute respiratory infections in subtropical China: an analysis over 11 years.Arch Virol. 2014 Apr;159(4):631-9. doi: 10.1007/s00705-013-1863-8. Epub 2013 Oct 10. Arch Virol. 2014. PMID: 24114148
-
Viral infections in relation to age, atopy, and season of admission among children hospitalized for wheezing.J Allergy Clin Immunol. 2004 Aug;114(2):239-47. doi: 10.1016/j.jaci.2004.04.006. J Allergy Clin Immunol. 2004. PMID: 15316497 Free PMC article.
-
Long-term effects of respiratory syncytial virus (RSV) bronchiolitis in infants and young children: a quantitative review.Acta Paediatr. 2000 Jun;89(6):654-60. doi: 10.1080/080352500750043945. Acta Paediatr. 2000. PMID: 10914957 Review.
-
Wheezing in children: Approaches to diagnosis and management.Int J Pediatr Adolesc Med. 2019 Jun;6(2):68-73. doi: 10.1016/j.ijpam.2019.02.003. Epub 2019 Mar 15. Int J Pediatr Adolesc Med. 2019. PMID: 31388550 Free PMC article. Review. No abstract available.
Cited by
-
Predicting monthly hospital outpatient visits based on meteorological environmental factors using the ARIMA model.Sci Rep. 2023 Feb 15;13(1):2691. doi: 10.1038/s41598-023-29897-y. Sci Rep. 2023. PMID: 36792764 Free PMC article.
-
Characteristics and trends of unintentional injuries among children and adolescents in Kunshan, China: a hospital-based retrospective study, 2018-2023.Front Public Health. 2025 Jun 11;13:1606347. doi: 10.3389/fpubh.2025.1606347. eCollection 2025. Front Public Health. 2025. PMID: 40567957 Free PMC article.
-
Study on the correlation between the number of mushroom poisoning cases and meteorological factors based on the generalized additive model in Guizhou Province, 2023.BMC Public Health. 2024 Sep 27;24(1):2628. doi: 10.1186/s12889-024-20050-6. BMC Public Health. 2024. PMID: 39333979 Free PMC article.
-
Referrals and Determinant Factors of a National School Health Campaign in Lebanon on Children Aged between 3 and 12 Years Old.Children (Basel). 2024 Jan 30;11(2):175. doi: 10.3390/children11020175. Children (Basel). 2024. PMID: 38397287 Free PMC article.
References
-
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2020. https://ginasthma.org/gina-reports/. (Accessed 14 June 2021).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
