

Culturally adapting internet- and mobile-based health promotion interventions might not be worth the effort: a systematic review and meta-analysis
- PMID: 35322172
- PMCID: PMC8943001
- DOI: 10.1038/s41746-022-00569-x
Culturally adapting internet- and mobile-based health promotion interventions might not be worth the effort: a systematic review and meta-analysis
Abstract
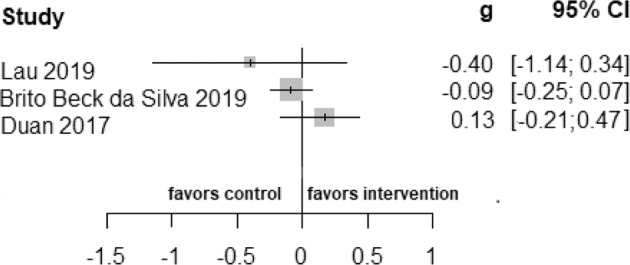
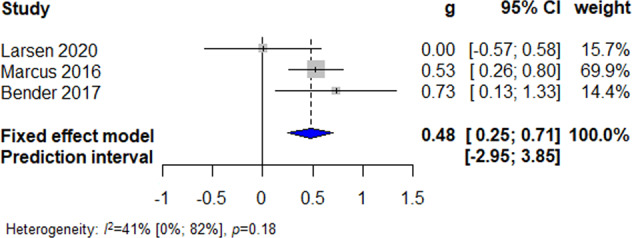
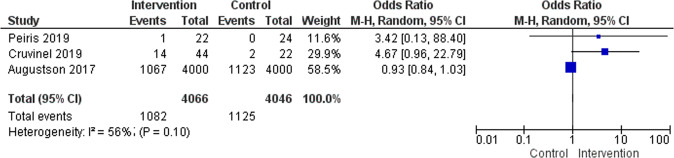
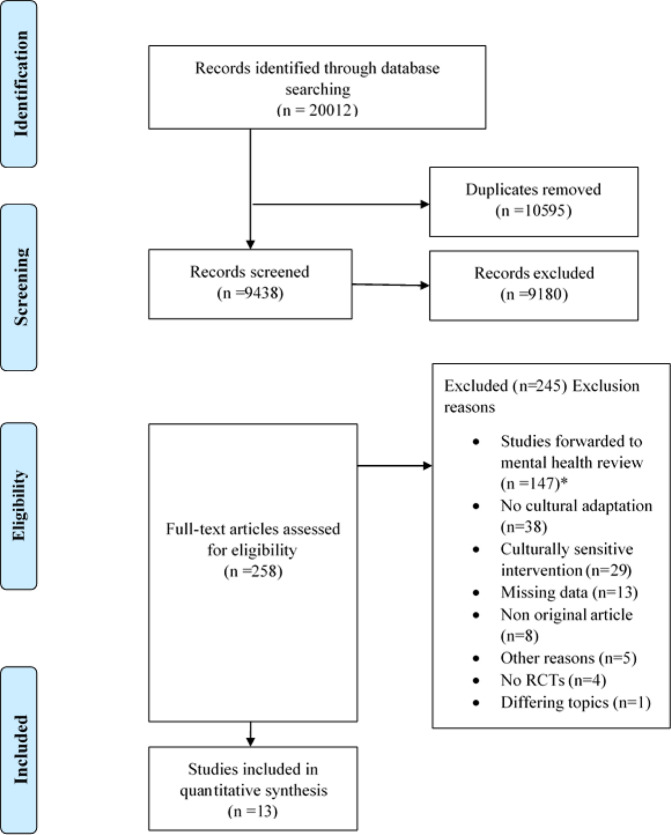
Health promotion interventions offer great potential in advocating a healthy lifestyle and the prevention of diseases. Some barriers to communicating health promotion to people of certain cultural groups might be overcome via the internet- and mobile-based interventions (IMI). This systematic review and meta-analysis aims to explore the effectiveness of culturally adapted IMI for health promotion interventions among culturally diverse populations. We systematically searched on Cochrane Central Register of Controlled Trials (CENTRAL), EbscoHost/MEDLINE, Ovid/Embase, EbscoHost/PsychINFO, and Web of Science databases in October 2020. Out of 9438 records, 13 randomized controlled trials (RCT) investigating culturally adapted health promotion IMI addressing healthy eating, physical activity, alcohol consumption, sexual health behavior, and smoking cessation included. From the included studies 10,747 participants were eligible. Culturally adapted IMI proved to be non-superior over active control conditions in short- (g = 0.10, [95% CI -0.19 to 0.40]) and long-term (g = 0.20, [95% CI -0.11 to 0.51]) in promoting health behavior. However, culturally adapted IMI for physical activity (k = 3, N = 296) compared to active controls yielded a beneficial effect in long-term (g = 0.48, [95%CI 0.25 to 0.71]). Adapting health promotion IMI to the cultural context of different cultural populations seems not yet to be recommendable given the substantial adaption efforts necessary and the mostly non-significant findings. However, these findings need to be seen as preliminary given the limited number of included trials with varying methodological rigor and the partly substantial between-trial heterogeneity pointing in the direction of potentially useful culturally adapted IMI which now need to be disentangled from the less promising approaches.PROSPERO registration number: 42020152939.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Cerf ME. Healthy lifestyles and noncommunicable diseases: nutrition, the life‐course, and health promotion. Lifestyle Med. 2021;2:1–12.
-
- World Health Organization. Sexual Health and its Linkages to Reproductive Health: an Operational Approach 1–12 (World Health Organization, 2017).
-
- Di Cesare M, et al. Inequalities in non-communicable diseases and effective responses. Lancet. 2013;381:585–597. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
