

Predictive factors of needle-knife pre-cut papillotomy failure in patients with difficult biliary cannulation
- PMID: 35322178
- PMCID: PMC8943021
- DOI: 10.1038/s41598-022-09117-9
Predictive factors of needle-knife pre-cut papillotomy failure in patients with difficult biliary cannulation
Abstract
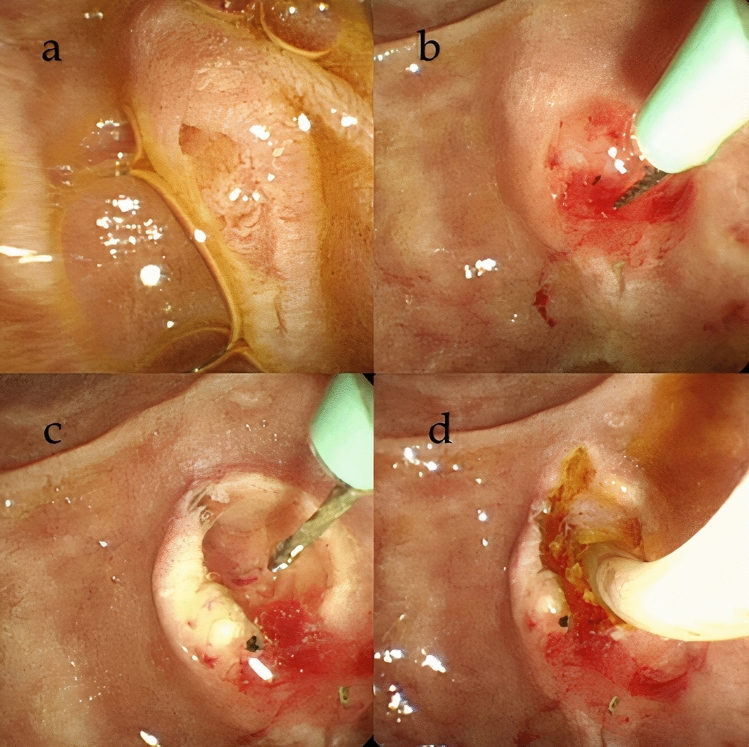
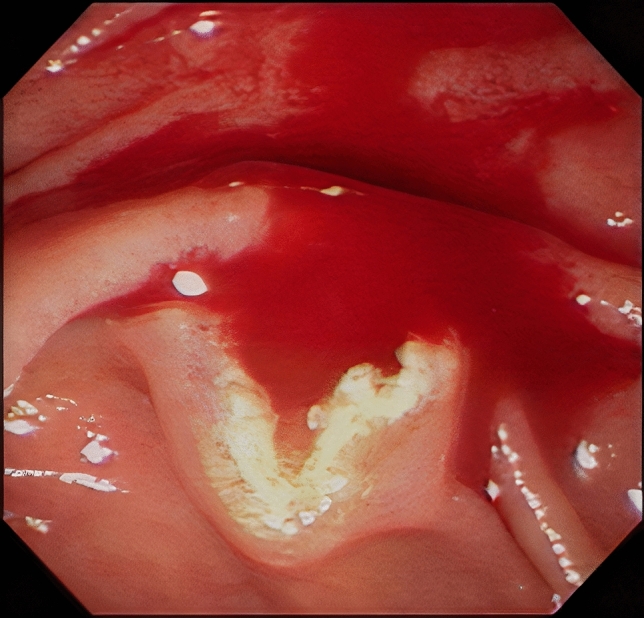
Predictors of needle-knife pre-cut papillotomy (NKP) failure for patients with difficult biliary cannulation has not been reported. Between 2004 and 2016, 390 patients with difficult biliary cannulation undergoing NKP were included in this single-center study. Following NKP, deep biliary cannulation failed in 95 patients (24.4%, NKP-failure group) and succeeded in 295 patients (75.6%, NKP-success group). Patient and technique factors were used to identify the predictors of initial NKP failure. Compared with the NKP-success group, periampullary diverticulum (28.4% vs. 18%, p = 0.028), surgically altered anatomy (13.7% vs. 7.1%, p = 0.049), number of cases performed by less experienced endoscopists, and bleeding during NKP (38.9% vs. 3.4%, p < 0.001), were significantly more frequent in the NKP-failure group. On multivariate analysis, surgically altered anatomy (OR 2.374, p = 0.045), endoscopists' experience (OR 3.593, p = 0.001), and bleeding during NKP (OR 21.18, p < 0.001) were significantly associated with initial failure of NKP. In conclusion, NKP is a highly technique-sensitive procedure, as endoscopists' experience, bleeding during NKP, and surgically altered anatomy were predictors of initial NKP failure.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Pancreatic stent improves the success rate of needle-knife papillotomy in patients with difficult biliary cannulation.World J Gastroenterol. 2025 Jan 7;31(1):97240. doi: 10.3748/wjg.v31.i1.97240. World J Gastroenterol. 2025. PMID: 39777249 Free PMC article.
-
Success and Safety of Needle Knife Papillotomy and Fistulotomy Based on Papillary Anatomy: A Prospective Controlled Trial.Dig Dis Sci. 2022 May;67(5):1901-1909. doi: 10.1007/s10620-021-06983-7. Epub 2021 Jun 3. Dig Dis Sci. 2022. PMID: 34081249 Clinical Trial.
-
The success rate of cannulation of needle-knife precut is superior to continuing wire-guided after difficult biliary cannulation with pancreatic stent placement.Surg Endosc. 2023 Apr;37(4):3253-3259. doi: 10.1007/s00464-023-09877-z. Epub 2023 Jan 16. Surg Endosc. 2023. PMID: 36645482
-
Comparison between Transpancreatic Sphincterotomy and Needle-Knife Precut in Difficult Cannulation of Endoscopic Retrograde Cholangiopancreatography: An Up-To-Date Meta-Analysis and Systematic Review.Dig Dis. 2023;41(2):304-315. doi: 10.1159/000528052. Epub 2022 Nov 16. Dig Dis. 2023. PMID: 36382645
-
Management of difficult or failed biliary access in initial ERCP: A review of current literature.Clin Res Hepatol Gastroenterol. 2019 Aug;43(4):365-372. doi: 10.1016/j.clinre.2018.09.004. Epub 2018 Oct 9. Clin Res Hepatol Gastroenterol. 2019. PMID: 30314736 Review.
Cited by
-
Pancreatic stent improves the success rate of needle-knife papillotomy in patients with difficult biliary cannulation.World J Gastroenterol. 2025 Jan 7;31(1):97240. doi: 10.3748/wjg.v31.i1.97240. World J Gastroenterol. 2025. PMID: 39777249 Free PMC article.
-
Does patient's position count during Endoscopic Retrograde Cholangio-pancreatography? Left lateral decubitus versus prone position.Pak J Med Sci. 2023 Sep-Oct;39(5):1232-1237. doi: 10.12669/pjms.39.5.6932. Pak J Med Sci. 2023. PMID: 37680842 Free PMC article.
-
Predictive factors of difficult biliary cannulation: An experience of a tunisian tertiary center.Heliyon. 2022 Dec 22;8(12):e12526. doi: 10.1016/j.heliyon.2022.e12526. eCollection 2022 Dec. Heliyon. 2022. PMID: 36619425 Free PMC article.
-
Does early application of needle-knife sphincterotomy (NKS) in patients with difficult biliary cannulation increase the risk of postERCP pancreatitis? A single centre study.Pak J Med Sci. 2023 May-Jun;39(3):698-703. doi: 10.12669/pjms.39.3.6777. Pak J Med Sci. 2023. PMID: 37250585 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
