

Automated artificial intelligence-based system for clinical follow-up of patients with age-related macular degeneration
- PMID: 35322564
- PMCID: PMC9790353
- DOI: 10.1111/aos.15133
Automated artificial intelligence-based system for clinical follow-up of patients with age-related macular degeneration
Abstract
Purpose: In this study, we investigate the potential of a novel artificial intelligence-based system for autonomous follow-up of patients treated for neovascular age-related macular degeneration (AMD).
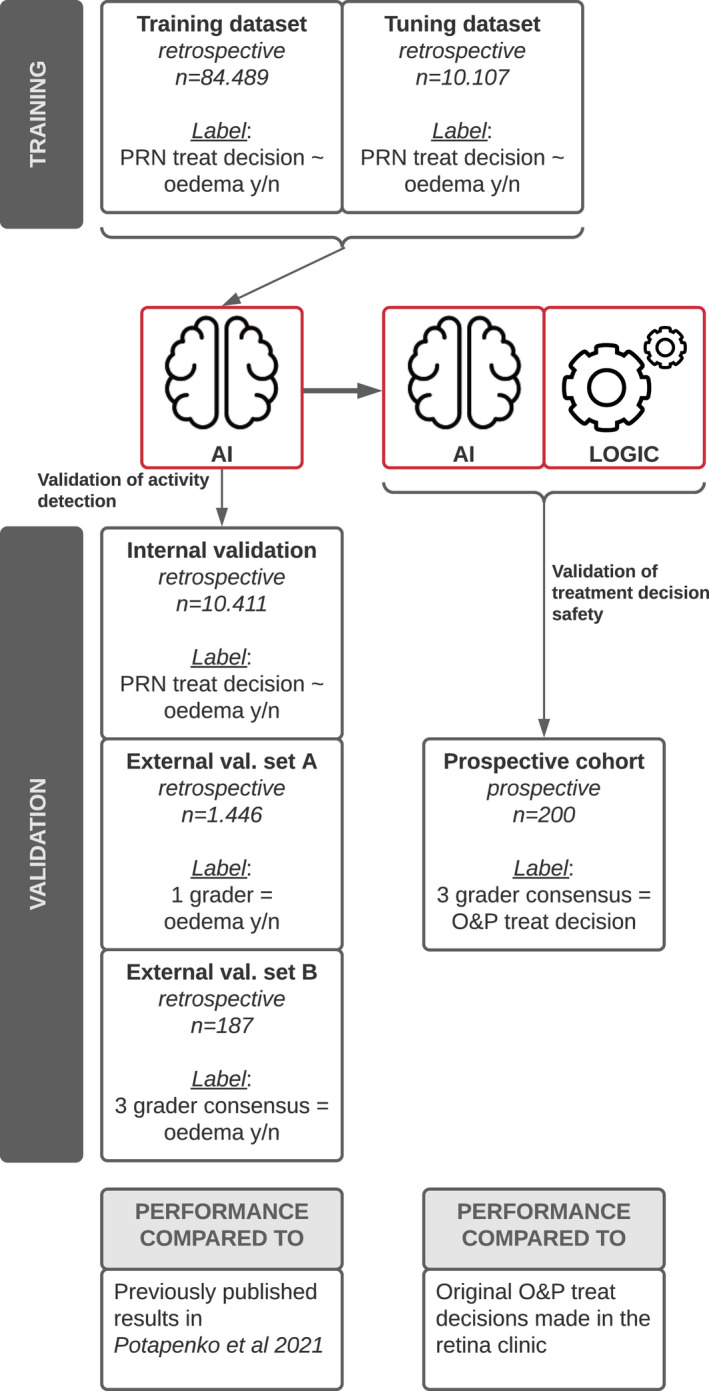
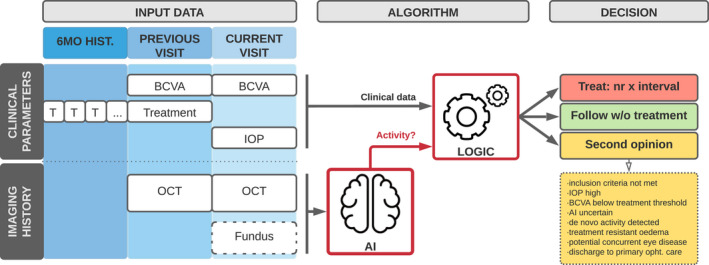
Methods: A temporal deep learning model was trained on a data set of 84 489 optical coherence tomography scans from AMD patients to recognize disease activity, and its performance was compared with a published non-temporal model trained on the same data (Acta Ophthalmol, 2021). An autonomous follow-up system was created by augmenting the AI model with deterministic logic to suggest treatment according to the observe-and-plan regimen. To validate the AI-based system, a data set comprising clinical decisions and imaging data from 200 follow-up consultations was collected prospectively. In each case, both the autonomous AI decision and original clinical decision were compared with an expert panel consensus.
Results: The temporal AI model proved superior at detecting disease activity compared with the model without temporal input (area under the curve 0.900 (95% CI 0.894-0.906) and 0.857 (95% CI 0.846-0.867) respectively). The AI-based follow-up system could make an autonomous decision in 73% of the cases, 91.8% of which were in agreement with expert consensus. This was on par with the 87.7% agreement rate between decisions made in the clinic and expert consensus (p = 0.33).
Conclusions: The proposed autonomous follow-up system was shown to be safe and compliant with expert consensus on par with clinical practice. The system could in the future ease the pressure on public ophthalmology services from an increasing number of AMD patients.
Keywords: age-related macular degeneration; anti-vegf; artificial intelligence; follow-up.
© 2022 The Authors. Acta Ophthalmologica published by John Wiley & Sons Ltd on behalf of Acta Ophthalmologica Scandinavica Foundation.
Figures
References
-
- Brown DM & Regillo CD (2007): Anti‐VEGF agents in the treatment of neovascular age‐related macular degeneration: applying clinical trial results to the treatment of everyday patients. Am J Ophthalmol 144: 627–637. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
