

Renal Artery Stenting in Consecutive High-Risk Patients With Atherosclerotic Renovascular Disease: A Prospective 2-Center Cohort Study
- PMID: 35322677
- PMCID: PMC9075498
- DOI: 10.1161/JAHA.121.024421
Renal Artery Stenting in Consecutive High-Risk Patients With Atherosclerotic Renovascular Disease: A Prospective 2-Center Cohort Study
Erratum in
-
Correction to: Renal Artery Stenting in Consecutive High-Risk Patients With Atherosclerotic Renovascular Disease: A Prospective 2-Center Cohort Study.J Am Heart Assoc. 2023 Apr 18;12(8):e020845. doi: 10.1161/JAHA.121.020845. Epub 2023 Apr 7. J Am Heart Assoc. 2023. PMID: 37026548 Free PMC article. No abstract available.
Abstract
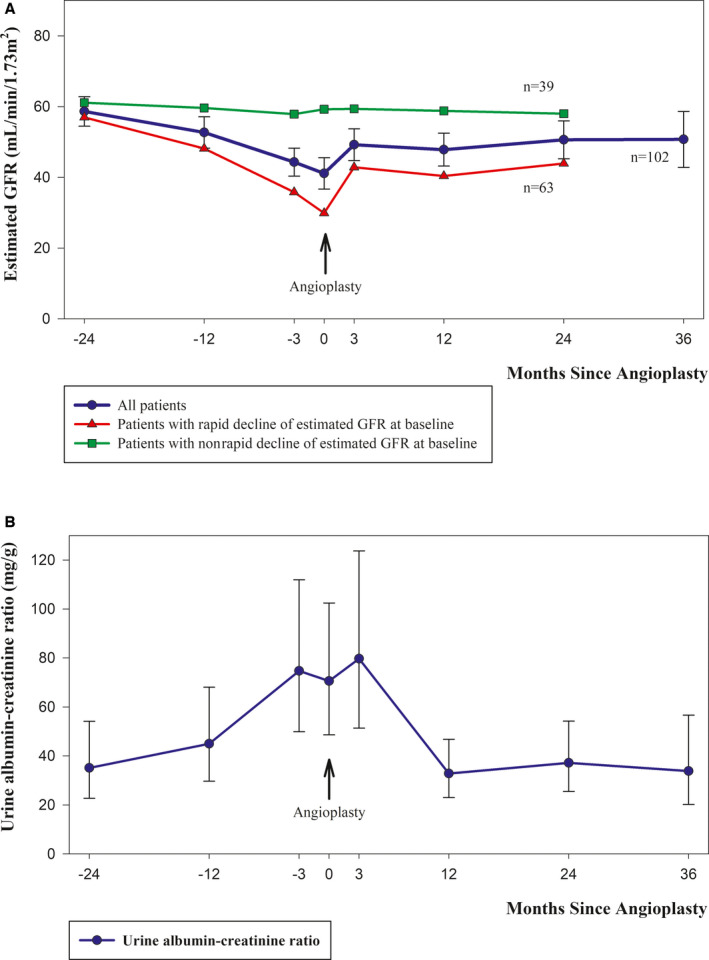
Background The aim of this study was to prospectively evaluate the effects of renal artery stenting in consecutive patients with severe atherosclerotic renal artery stenosis and high-risk clinical presentations as defined in a national protocol developed in 2015. Methods and Results Since the protocol was initiated, 102 patients have been referred for revascularization according to the following high-risk criteria: severe renal artery stenosis (≥70%) with true resistant hypertension, rapidly declining kidney function, or recurrent heart failure/sudden pulmonary edema. At baseline, the mean 24-hour ambulatory systolic blood pressure was 166.2 mm Hg (95% CI, 162.0-170.4), the defined daily dose of antihypertensive medication was 6.5 (95% CI, 5.8-7.3), and the estimated glomerular filtration rate was 41.1 mL/min per 1.73m2 (95% CI, 36.6-45.6). In 96 patients with available 3-month follow-up data, mean 24-hour ambulatory systolic blood pressure decreased by 19.6 mm Hg (95% CI, 15.4-23.8; P<0.001), the defined daily dose of antihypertensive medication was reduced by 52% (95% CI, 41%-62%; P<0.001), and estimated glomerular filtration rate increased by 7.8 mL/min per 1.73m2 (95% CI, 4.5-11.1; P<0.001). All changes persisted after 24 month follow-up. Among 17 patients with a history of hospitalization for acute decompensated heart failure, 14 patients had no new episodes after successful revascularization. Conclusions In this prospective cohort study, we observed a reduction in blood pressure and antihypertensive medication, an increase in estimated glomerular filtration rate, and a decrease in new hospital admissions attributable to heart failure/sudden pulmonary edema after renal artery stenting. Registration URL: https://clinicaltrials.gov. Identifier: NCT02770066.
Keywords: atherosclerotic renal artery stenosis; atherosclerotic renovascular disease; flash pulmonary edema; rapid loss of kidney function; renal revascularization; resistant hypertension.
Figures


Comment in
-
Cardiovascular Disease Prevention in Patients With Atherosclerotic Renovascular Disease-Induced Resistant Hypertension: Further Considerations for 24-Hour Blood Pressure Profiles.J Am Heart Assoc. 2022 Sep 6;11(17):e025901. doi: 10.1161/JAHA.122.025901. Epub 2022 Aug 17. J Am Heart Assoc. 2022. PMID: 35975740 Free PMC article. No abstract available.
-
Vini Vidi Stenti.J Am Heart Assoc. 2022 Sep 6;11(17):e025900. doi: 10.1161/JAHA.122.025900. Epub 2022 Aug 17. J Am Heart Assoc. 2022. PMID: 35975744 Free PMC article. No abstract available.
References
-
- Bax L, Woittiez AJ, Kouwenberg HJ, Mali WP, Buskens E, Beek FJ, Braam B, Huysmans FT, Schultze Kool LJ, Rutten MJ, et al. Stent placement in patients with atherosclerotic renal artery stenosis and impaired renal function: a randomized trial. Ann Intern Med. 2009;150:840–841. doi: 10.7326/0003-4819-150-12-200906160-00119 - DOI - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
