

Multiclass Arrhythmia Detection and Classification From Photoplethysmography Signals Using a Deep Convolutional Neural Network
- PMID: 35322685
- PMCID: PMC9075456
- DOI: 10.1161/JAHA.121.023555
Multiclass Arrhythmia Detection and Classification From Photoplethysmography Signals Using a Deep Convolutional Neural Network
Abstract
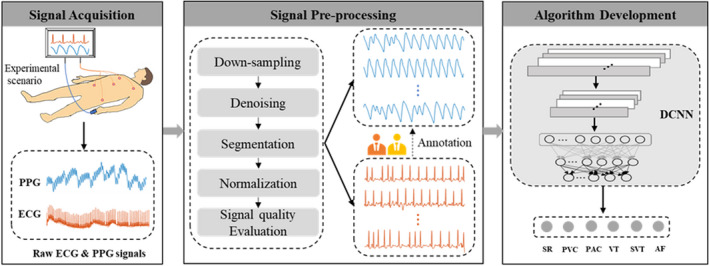
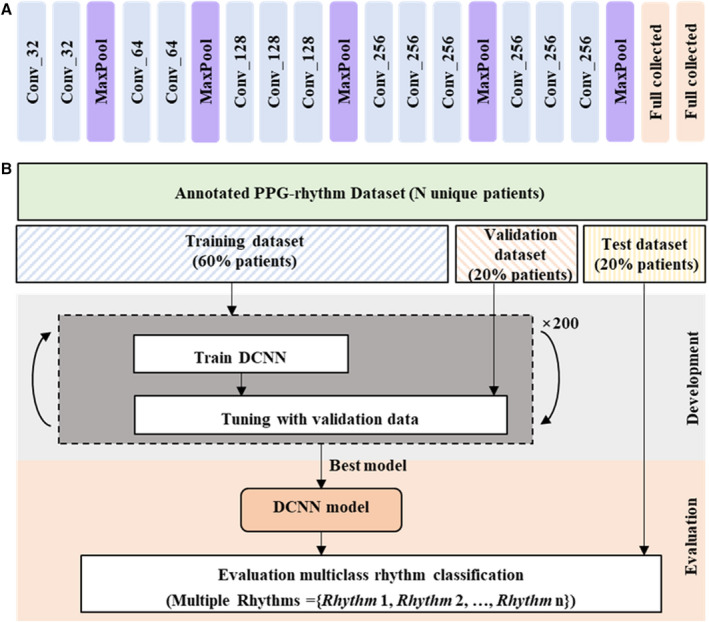
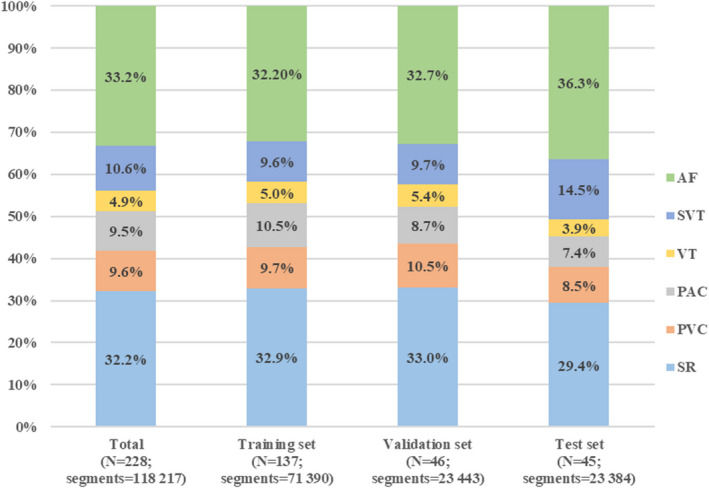
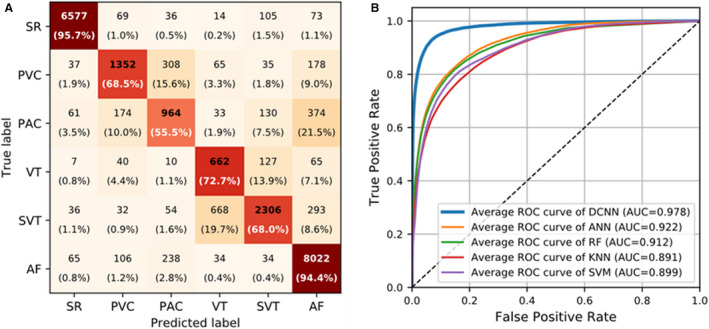
Background Studies have reported the use of photoplethysmography signals to detect atrial fibrillation; however, the use of photoplethysmography signals in classifying multiclass arrhythmias has rarely been reported. Our study investigated the feasibility of using photoplethysmography signals and a deep convolutional neural network to classify multiclass arrhythmia types. Methods and Results ECG and photoplethysmography signals were collected simultaneously from a group of patients who underwent radiofrequency ablation for arrhythmias. A deep convolutional neural network was developed to classify multiple rhythms based on 10-second photoplethysmography waveforms. Classification performance was evaluated by calculating the area under the microaverage receiver operating characteristic curve, overall accuracy, sensitivity, specificity, and positive and negative predictive values against annotations on the rhythm of arrhythmias provided by 2 cardiologists consulting the ECG results. A total of 228 patients were included; 118 217 pairs of 10-second photoplethysmography and ECG waveforms were used. When validated against an independent test data set (23 384 photoplethysmography waveforms from 45 patients), the DCNN achieved an overall accuracy of 85.0% for 6 rhythm types (sinus rhythm, premature ventricular contraction, premature atrial contraction, ventricular tachycardia, supraventricular tachycardia, and atrial fibrillation); the microaverage area under the microaverage receiver operating characteristic curve was 0.978; the average sensitivity, specificity, and positive and negative predictive values were 75.8%, 96.9%, 75.2%, and 97.0%, respectively. Conclusions This study demonstrated the feasibility of classifying multiclass arrhythmias from photoplethysmography signals using deep learning techniques. The approach is attractive for population-based screening and may hold promise for the long-term surveillance and management of arrhythmia. Registration URL: www.chictr.org.cn. Identifier: ChiCTR2000031170.
Keywords: arrhythmias; deep convolutional neural networks; photoplethysmography.
Figures
Similar articles
-
Diagnostic assessment of a deep learning system for detecting atrial fibrillation in pulse waveforms.Heart. 2018 Dec;104(23):1921-1928. doi: 10.1136/heartjnl-2018-313147. Epub 2018 May 31. Heart. 2018. PMID: 29853485
-
A CNN and Transformer Hybrid Network for Multi-Class Arrhythmia Detection from Photoplethysmography.Annu Int Conf IEEE Eng Med Biol Soc. 2024 Jul;2024:1-5. doi: 10.1109/EMBC53108.2024.10782549. Annu Int Conf IEEE Eng Med Biol Soc. 2024. PMID: 40031449
-
Multiclass Convolutional Neural Networks for Atrial Fibrillation Classification.Annu Int Conf IEEE Eng Med Biol Soc. 2022 Jul;2022:1288-1291. doi: 10.1109/EMBC48229.2022.9871124. Annu Int Conf IEEE Eng Med Biol Soc. 2022. PMID: 36086141
-
Review of Deep Learning-Based Atrial Fibrillation Detection Studies.Int J Environ Res Public Health. 2021 Oct 28;18(21):11302. doi: 10.3390/ijerph182111302. Int J Environ Res Public Health. 2021. PMID: 34769819 Free PMC article. Review.
-
Systematic Review on Features Extracted from PPG Signals for the Detection of Atrial Fibrillation.Stud Health Technol Inform. 2019;261:266-273. Stud Health Technol Inform. 2019. PMID: 31156128
Cited by
-
A Dual-Modal Wearable Pulse Detection System Integrated with Deep Learning for High-Accuracy and Low-Power Sleep Apnea Monitoring.Adv Sci (Weinh). 2025 Jun;12(24):e2501750. doi: 10.1002/advs.202501750. Epub 2025 Apr 29. Adv Sci (Weinh). 2025. PMID: 40298874 Free PMC article.
-
FMCW-based contactless heart rate monitoring.Sci Rep. 2025 Jan 21;15(1):2616. doi: 10.1038/s41598-025-86438-5. Sci Rep. 2025. PMID: 39837909 Free PMC article.
-
Multiclass arrhythmia classification using multimodal smartwatch photoplethysmography signals collected in real-life settings.Res Sq [Preprint]. 2024 Dec 13:rs.3.rs-5463126. doi: 10.21203/rs.3.rs-5463126/v1. Res Sq. 2024. PMID: 39711547 Free PMC article. Preprint.
-
Leveraging Classifier Performance Using Heuristic Optimization for Detecting Cardiovascular Disease from PPG Signals.Diagnostics (Basel). 2024 Oct 14;14(20):2287. doi: 10.3390/diagnostics14202287. Diagnostics (Basel). 2024. PMID: 39451610 Free PMC article.
-
Machine Learning Techniques for the Performance Enhancement of Multiple Classifiers in the Detection of Cardiovascular Disease from PPG Signals.Bioengineering (Basel). 2023 Jun 2;10(6):678. doi: 10.3390/bioengineering10060678. Bioengineering (Basel). 2023. PMID: 37370609 Free PMC article.
References
-
- Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, D’Agostino RB, Murabito JM, Kannel WB, Benjamin EJ. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the framingham heart study. Circulation. 2003;107:2920–2925. doi: 10.1161/01.CIR.0000072767.89944.6E - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
