

SGLT2 Inhibition and Uric Acid Excretion in Patients with Type 2 Diabetes and Normal Kidney Function
- PMID: 35322793
- PMCID: PMC9269569
- DOI: 10.2215/CJN.11480821
SGLT2 Inhibition and Uric Acid Excretion in Patients with Type 2 Diabetes and Normal Kidney Function
Abstract
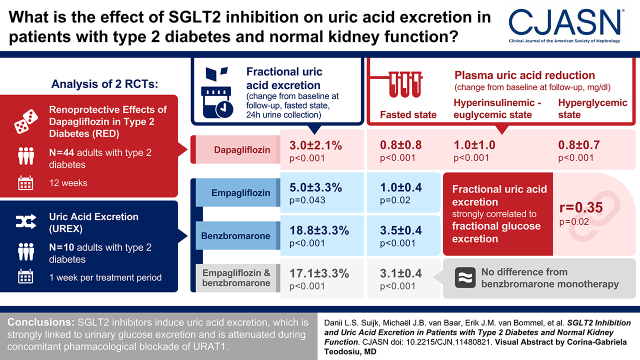
Background and objectives: Sodium-glucose transporter 2 (SGLT2) inhibitor-induced uric acid lowering may contribute to kidney-protective effects of the drug class in people with type 2 diabetes. This study investigates mechanisms of plasma uric acid lowering by SGLT2 inhibitors in people with type 2 diabetes with a focus on urate transporter 1.
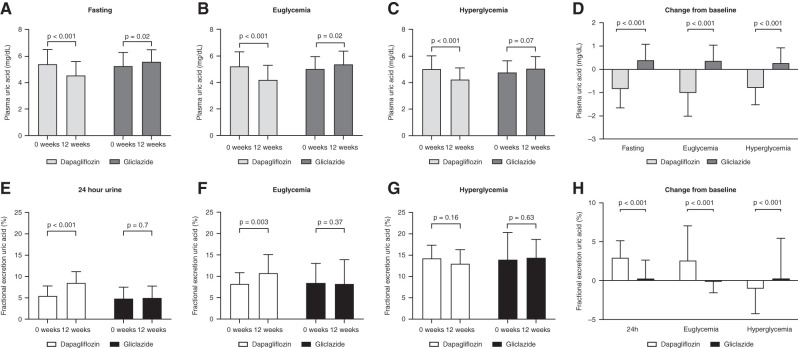
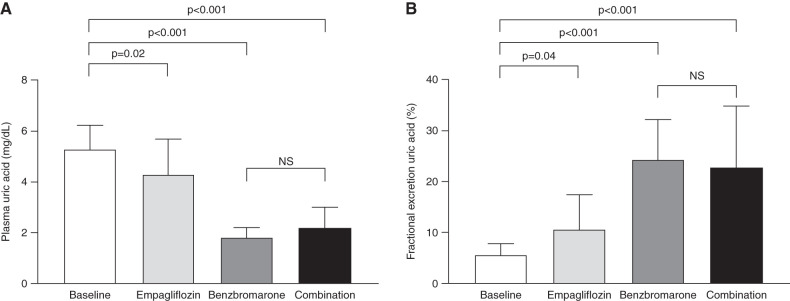
Design, setting, participants, & measurements: We conducted an analysis of two randomized clinical trials. First, in the Renoprotective Effects of Dapagliflozin in Type 2 Diabetes study, 44 people with type 2 diabetes were randomized to dapagliflozin or gliclazide for 12 weeks. Plasma uric acid, fractional uric acid excretion, and hemodynamic kidney function were measured in the fasted state and during clamped euglycemia or hyperglycemia. Second, in the Uric Acid Excretion study, ten people with type 2 diabetes received 1 week of empagliflozin, urate transporter 1 blocker benzbromarone, or their combination in a crossover design, and effects on plasma uric acid, fractional uric acid excretion, and 24-hour uric acid excretion were measured.
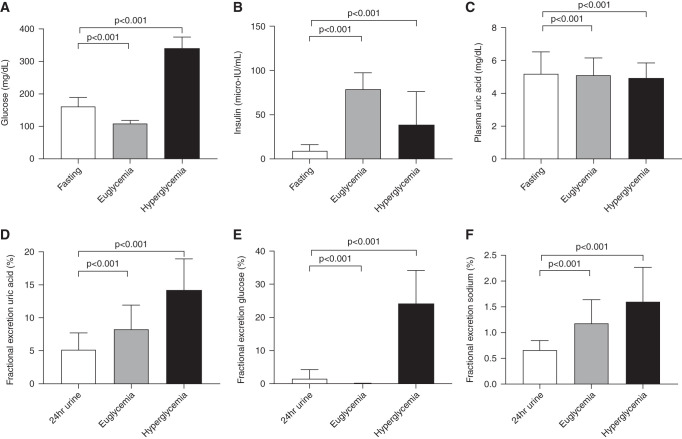
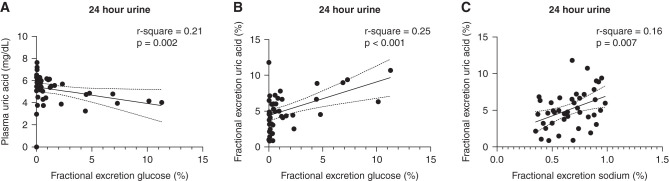
Results: In the Renoprotective Effects of Dapagliflozin in Type 2 Diabetes study, compared with the fasted state (5.3±1.1 mg/dl), acute hyperinsulinemia and hyperglycemia significantly reduced plasma uric acid by 0.2±0.3 and 0.4±0.3 mg/dl (both P<0.001) while increasing fractional uric acid excretion (by 3.2%±3.1% and 8.9%±4.5%, respectively; both P<0.001). Dapagliflozin reduced plasma uric acid by 0.8±0.8 during fasting, 1.0±1.0 in hyperinsulinemic-euglycemic state, and 0.8±0.7 mg/dl during hyperglycemic conditions (P<0.001), respectively, whereas fractional uric acid excretion in 24-hour urine increased by 3.0%±2.1% (P<0.001) and 2.6%±4.5% during hyperinsulinemic-euglycemic conditions (P=0.003). Fractional uric acid excretion strongly correlated to fractional glucose excretion (r=0.35; P=0.02). In the Uric Acid Excretion study, empagliflozin and benzbromarone both significantly reduced plasma uric acid and increased fractional uric acid excretion. Effects of combination therapy did not differ from benzbromarone monotherapy.
Conclusions: In conclusion, SGLT2 inhibitors induce uric acid excretion, which is strongly linked to urinary glucose excretion and is attenuated during concomitant pharmacologic blockade of urate transporter 1.
Clinical trial registry name and registration number: Renoprotective Effects of Dapagliflozin in Type 2 Diabetes (RED), NCT02682563; SGLT2 Inhibition: Uric Acid Excretion Study (UREX), NCT05210517.
Keywords: SGLT-2 inhibition; URAT-1; kidney; type 2 diabetes; uric acid.
Copyright © 2022 by the American Society of Nephrology.
Figures
References
-
- Johnson RJ, Bakris GL, Borghi C, Chonchol MB, Feldman D, Lanaspa MA, Merriman TR, Moe OW, Mount DB, Sanchez Lozada LG, Stahl E, Weiner DE, Chertow GM: Hyperuricemia, acute and chronic kidney disease, hypertension, and cardiovascular disease: Report of a scientific workshop organized by the National Kidney Foundation. Am J Kidney Dis 71: 851–865, 2018 - PMC - PubMed
-
- Sato Y, Feig DI, Stack AG, Kang DH, Lanaspa MA, Ejaz AA, Sánchez-Lozada LG, Kuwabara M, Borghi C, Johnson RJ: The case for uric acid-lowering treatment in patients with hyperuricaemia and CKD. Nat Rev Nephrol 15: 767–775, 2019 - PubMed
-
- Doria A, Galecki AT, Spino C, Pop-Busui R, Cherney DZ, Lingvay I, Parsa A, Rossing P, Sigal RJ, Afkarian M, Aronson R, Caramori ML, Crandall JP, de Boer IH, Elliott TG, Goldfine AB, Haw JS, Hirsch IB, Karger AB, Maahs DM, McGill JB, Molitch ME, Perkins BA, Polsky S, Pragnell M, Robiner WN, Rosas SE, Senior P, Tuttle KR, Umpierrez GE, Wallia A, Weinstock RS, Wu C, Mauer M; PERL Study Group : Serum urate lowering with allopurinol and kidney function in type 1 diabetes. N Engl J Med 382: 2493–2503, 2020 - PMC - PubMed
-
- Badve SV, Pascoe EM, Tiku A, Boudville N, Brown FG, Cass A, Clarke P, Dalbeth N, Day RO, de Zoysa JR, Douglas B, Faull R, Harris DC, Hawley CM, Jones GRD, Kanellis J, Palmer SC, Perkovic V, Rangan GK, Reidlinger D, Robison L, Walker RJ, Walters G, Johnson DW; CKD-FIX Study Investigators : Effects of allopurinol on the progression of chronic kidney disease. N Engl J Med 382: 2504–2513, 2020 - PubMed
-
- Zhao Y, Xu L, Tian D, Xia P, Zheng H, Wang L, Chen L: Effects of sodium-glucose co-transporter 2 (SGLT2) inhibitors on serum uric acid level: A meta-analysis of randomized controlled trials. Diabetes Obes Metab 20: 458–462, 2018 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
