

A model based on endorectal ultrasonography predicts lateral lymph node metastasis in low and middle rectal cancer
- PMID: 35322883
- PMCID: PMC9313894
- DOI: 10.1002/jcu.23204
A model based on endorectal ultrasonography predicts lateral lymph node metastasis in low and middle rectal cancer
Abstract
Purpose: To investigate the risk factors for lymph node (LN) metastasis in low and middle rectal tumors, construct a predictive model and test the model's diagnostic efficacy.
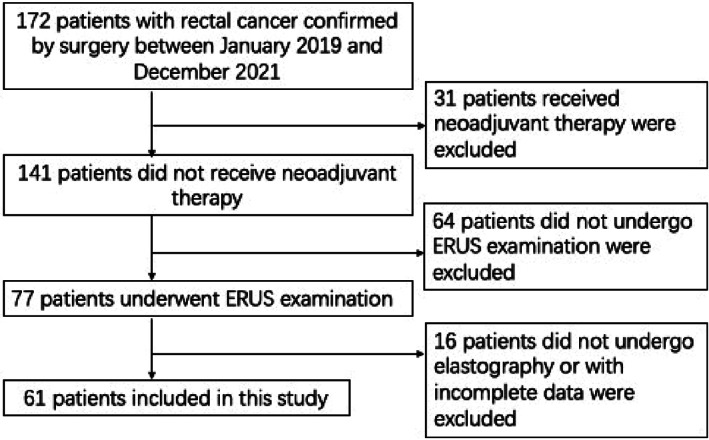
Methods: The clinical and pathological data of 172 patients with rectal cancer confirmed by surgery were retrospectively evaluated, among whom 61 patients were finally included in this study. Patients were divided into positive groups and negative groups based on LN metastasis, and risk factors that might affect LN metastasis were analyzed. Finally, a risk predictive model was constructed based on the weights of each risk factor.
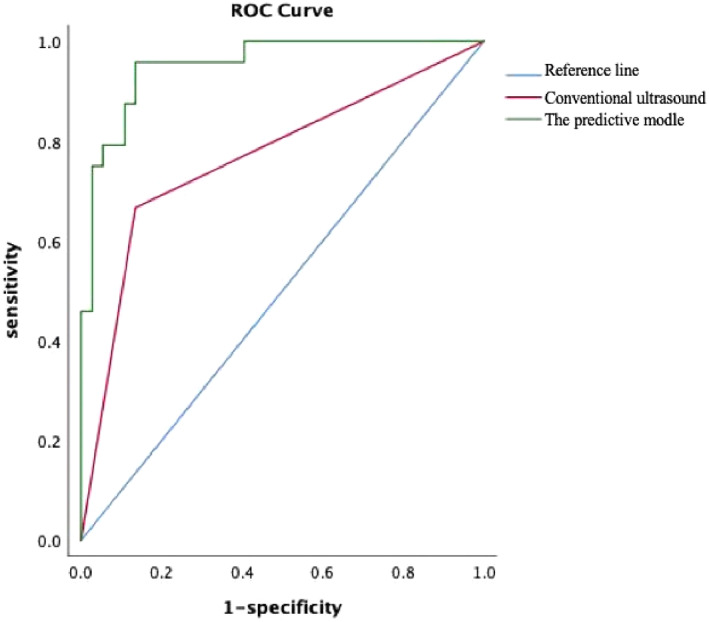
Results: Compared with pathology, the efficacy of diagnosing LN metastasis only according to conventional endorectal ultrasonography (ERUS) features of LN was not high, with sensitivity 67%, specificity 86%, positive predictive value 76%, negative predictive value 80%, and accuracy 79%. Univariate analysis showed that circumferential angle of the tumor, ultrasonic T- stage (UT stage), conventional ultrasound features diagnosis of LN metastasis, strain ratio (SR) of tumor were risk factors for LN metastasis, while vascular resistance index of rectal tumor was protective factor. Multivariate analysis showed that UT stage (OR = 7.188, p = 0.049), conventional ultrasound features diagnosis of LN metastasis (OR = 8.010, p = 0.025) and SR (OR = 5.022, p = 0.031) were independent risk factors for LN metastasis. These risk factors were included in logistic regression analysis and the model was established, Y = -7.3 + 1.9 X10 + 2.1 X11 + 1.6 X13 (Y = Logit[P], P: LN metastasis rate, X10: UT stage, X11: conventional ultrasound features diagnosis of LN metastasis, X13: SR). The receiver operating characteristic (ROC) curve was used to test the model's predictive efficacy, the area under the curve was 0.95, sensitivity: 95%, specificity: 87%. Hosmer-Lemeshow goodness of fit test showed X2 = 6.015, p = 0.65 (p > 0.05), indicating that the model had a high predictive value.
Conclusion: Evaluation of perirectal LN metastasis only based on conventional ERUS features of LN was not effective enough. UT stage of tumor, conventional ultrasound features diagnosis of LN metastasis and SR were independent risk factors for LN metastasis. The predictive model had good assessment efficacy and had certain clinical application value.
Keywords: ERUS; SR; lymph node metastasis; rectal cancer.
© 2022 The Authors. Journal of Clinical Ultrasound published by Wiley Periodicals LLC.
Conflict of interest statement
The author has no conflict of interest to disclose.
Figures
Similar articles
-
Utility of Machine Learning Algorithms in Predicting Preoperative Lymph Node Metastasis in Patients With Rectal Cancer Based on Three-Dimensional Endorectal Ultrasound and Clinical and Laboratory Data.J Ultrasound Med. 2023 Nov;42(11):2615-2627. doi: 10.1002/jum.16297. Epub 2023 Jul 4. J Ultrasound Med. 2023. PMID: 37401518
-
[MRI associated biomarker analysis for diagnosis of lymph node metastasis in T1-2 stage rectal cancer].Zhonghua Zhong Liu Za Zhi. 2021 Feb 23;43(2):207-212. doi: 10.3760/cma.j.cn112152-20200429-00391. Zhonghua Zhong Liu Za Zhi. 2021. PMID: 33601486 Chinese.
-
Accuracy of F-18 FDG PET/CT with optimal cut-offs of maximum standardized uptake value according to size for diagnosis of regional lymph node metastasis in patients with rectal cancer.Cancer Imaging. 2018 Sep 14;18(1):32. doi: 10.1186/s40644-018-0165-5. Cancer Imaging. 2018. PMID: 30217167 Free PMC article.
-
Endorectal ultrasound in the preoperative evaluation of rectal cancer.Clin Colorectal Cancer. 2004 Jul;4(2):124-32. doi: 10.3816/ccc.2004.n.015. Clin Colorectal Cancer. 2004. PMID: 15285819 Review.
-
Revolutionizing lymph node metastasis imaging: the role of drug delivery systems and future perspectives.J Nanobiotechnology. 2024 Mar 29;22(1):135. doi: 10.1186/s12951-024-02408-5. J Nanobiotechnology. 2024. PMID: 38553735 Free PMC article. Review.
Cited by
-
Predictive Value of TRUS and CEUS Parameters for Lymph Node Metastasis in Rectal Cancer: A Retrospective Study.Int J Gen Med. 2025 Jun 24;18:3335-3345. doi: 10.2147/IJGM.S519039. eCollection 2025. Int J Gen Med. 2025. PMID: 40585581 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7‐34. - PubMed
-
- Sobin LH, Wittekind C. International Union Against Cancer (UICC) TNM Classification of Malignant Tumours. 6th ed. Wiley‐Liss; 2002:99‐103.
-
- Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population‐based to a more "personalized" approach to cancer staging. CA Cancer J Clin. 2017;67:93‐99. - PubMed
-
- Kim E, Hwang JM, Garcia‐Aguilar J. Local excision for rectal carcinoma. Clin Colorectal Cancer. 2008;7:376‐385. - PubMed
-
- Beddy D, Hyland JMP, Winter DC, et al. A simplified tumor regression grade correlates with survival in locally advanced rectal carcinoma treated with neoadjuvant chemotherapy. Ann Surg Oncol. 2008;15:3471‐3477. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
