

Reduction of Hospitalization and Mortality by Echocardiography-Guided Treatment in Advanced Heart Failure
- PMID: 35323622
- PMCID: PMC8953534
- DOI: 10.3390/jcdd9030074
Reduction of Hospitalization and Mortality by Echocardiography-Guided Treatment in Advanced Heart Failure
Abstract
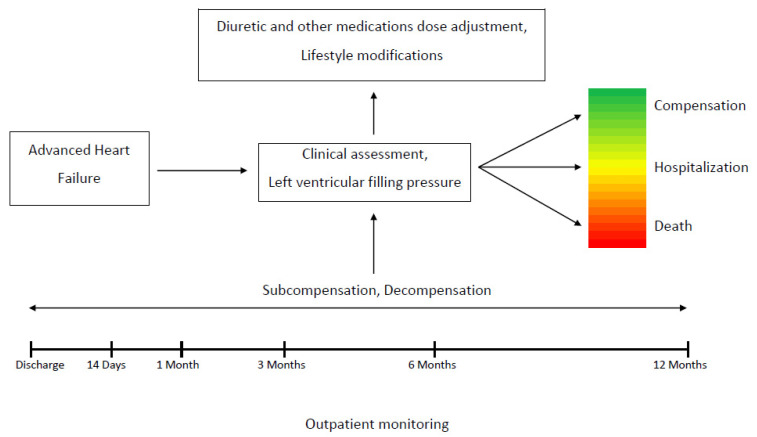
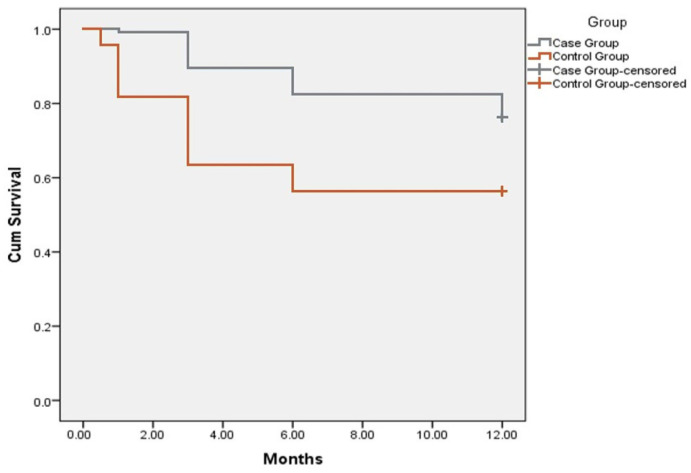
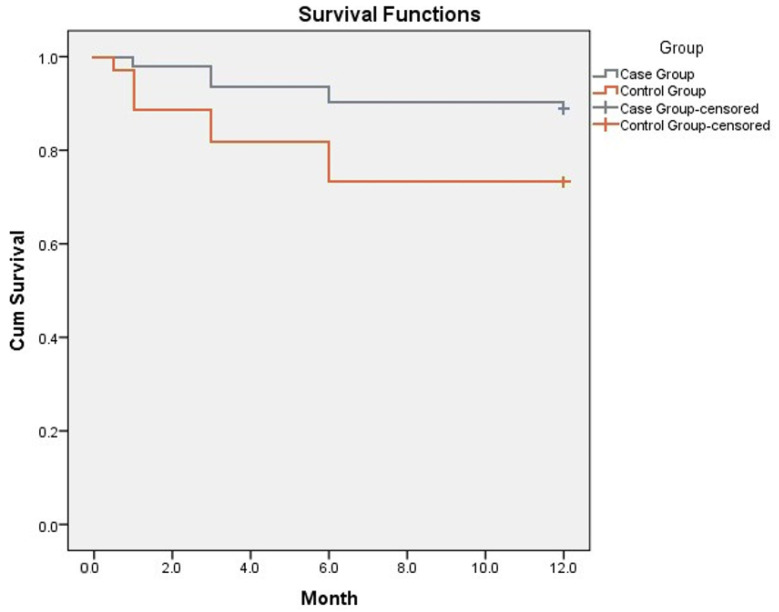
In advanced heart failure (AHF) clinical evaluation fails to detect subclinical HF deterioration in outpatient settings. The aim of the study was to determine whether the strategy of intensive outpatient echocardiographic monitoring, followed by treatment modification, reduces mortality and re-hospitalizations at 12 months. Methods: 214 patients with ejection fraction < 30% and >1 hospitalization during the last year underwent clinical evaluation and echocardiography at discharge and were divided into intensive (IMG; N = 143) or standard monitoring group (SMG; N = 71). In IMG, volemic status and left ventricular filling pressure were assessed 14, 30, 90, 180 and 365 days after discharge. HF treatment, particularly diuretic therapy, was temporarily intensified when HF deterioration signs and E/e’ > 15 were detected. In SMG, standard outpatient monitoring without obligatory echocardiography at outpatient visits was performed. Results: We observed lower hospitalization (absolute risk reduction [ARR]-0.343, CI-95%: 0.287−0.434, p < 0.05; number needed to treat [NNT]-2.91) and mortality (ARR-0.159, CI 95%: 0.127−0.224, p < 0.05; NNT-6.29) in IMG at 12 months. One-year survival was 88.8% in IMG and 71.8% in SMG (p < 0.05). Conclusion: In AHF, outpatient monitoring of volemic status and intracardiac filling pressures to individualize treatment may potentially reduce hospitalizations and mortality at 12 months follow-up. Echocardiography-guided outpatient therapy is feasible and clinically beneficial, providing evidence for the larger application of this approach.
Keywords: Tissue Doppler echocardiography; advanced heart failure; left ventricular filling pressure; mortality; outpatient monitoring; rehospitalizations.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Yancy C.W., Jessup M., Bozkurt B., Butler J., Casey D.E., Jr., Drazner M.H., Fonarow G.C., Geraci S.A., Horwich T., Januzzi J.L., et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A report of the American College of Cardiology Founda-tion/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013;62:e147–e239. doi: 10.1016/j.jacc.2013.05.019. - DOI - PubMed
-
- Crespo-Leiro M.G., Metra M., Lund L.H., Milicic D., Costanzo M.R., Filippatos G., Gustafsson F., Tsui S., Barge-Caballero E., De Jonge N., et al. Advanced heart failure: A position statement of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018;20:1505–1535. doi: 10.1002/ejhf.1236. - DOI - PubMed
-
- Metra M., Ponikowski P., Dickstein K., McMurray J.J., Gavazzi A., Bergh C.-H., Fraser A.G., Jaarsma T., Pitsis A., Mohacsi P., et al. Advanced chronic heart failure: A position statement from the Study Group on Advanced Heart Failure of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2007;9:684–694. doi: 10.1016/j.ejheart.2007.04.003. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
