

Kisspeptin Overcomes GnRH Neuronal Suppression Secondary to Hyperprolactinemia in Humans
- PMID: 35323937
- PMCID: PMC9282259
- DOI: 10.1210/clinem/dgac166
Kisspeptin Overcomes GnRH Neuronal Suppression Secondary to Hyperprolactinemia in Humans
Erratum in
-
Correction to: Kisspeptin Overcomes GnRH Neuronal Suppression Secondary to Hyperprolactinemia in Humans.J Clin Endocrinol Metab. 2022 Jul 14;107(8):e3543. doi: 10.1210/clinem/dgac302. J Clin Endocrinol Metab. 2022. PMID: 35584786 Free PMC article. No abstract available.
Abstract
Context: Hyperprolactinemia suppresses gonadotropin-releasing hormone (GnRH)-induced luteinizing hormone (LH) pulses. The hypothalamic neuropeptide kisspeptin potently stimulates the secretion of GnRH. The effects of exogenous kisspeptin administration on GnRH pulse generation in the setting of hyperprolactinemia have not previously been explored.
Objective: This work aimed to examine the effects of kisspeptin on GnRH secretion, as reflected by LH secretion, in women with hyperprolactinemia.
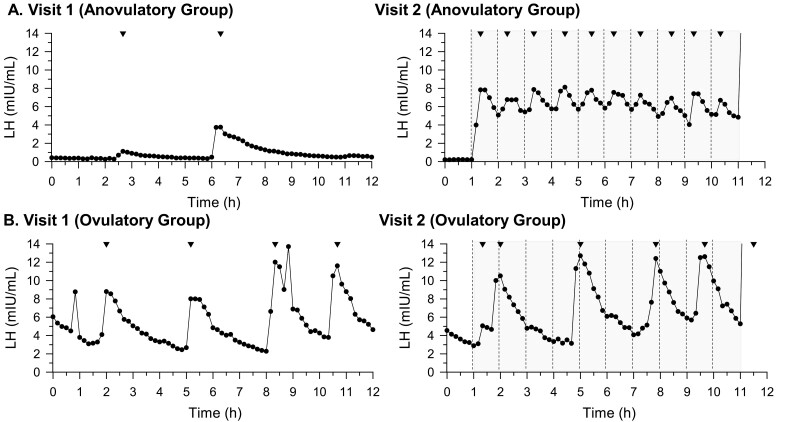
Methods: Women with hyperprolactinemia (n = 11) participated in two 12-hour visits. Before study visits, participants underwent washout of dopamine agonist and/or combined oral contraceptive. Frequent blood sampling was performed (1 sample was collected every 10 minutes). Visit 1 involved no intervention, to examine baseline LH pulsatility. During visit 2, kisspeptin 112-121 (0.24 nmol/kg) was administered every 1 hour, for 10 hours. At hour 11, one intravenous bolus of GnRH (75 ng/kg) was administered.
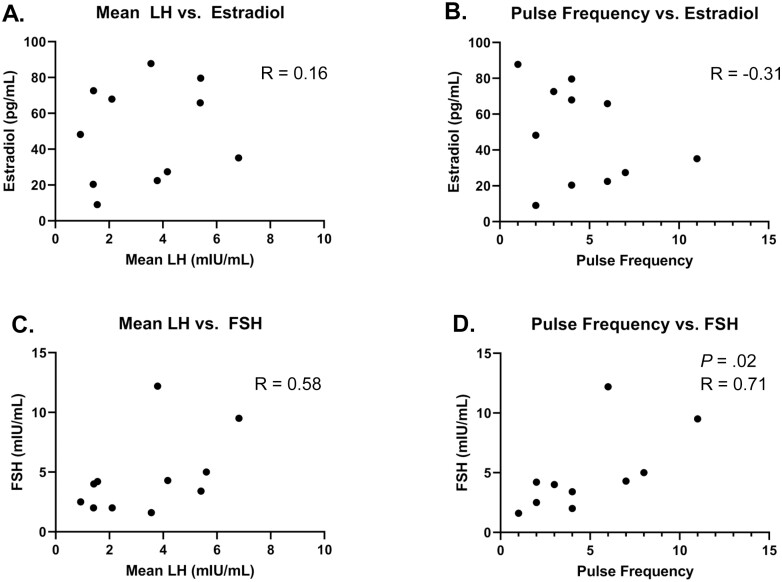
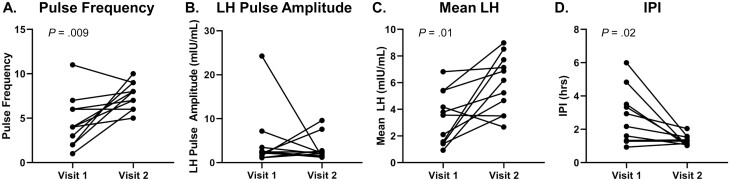
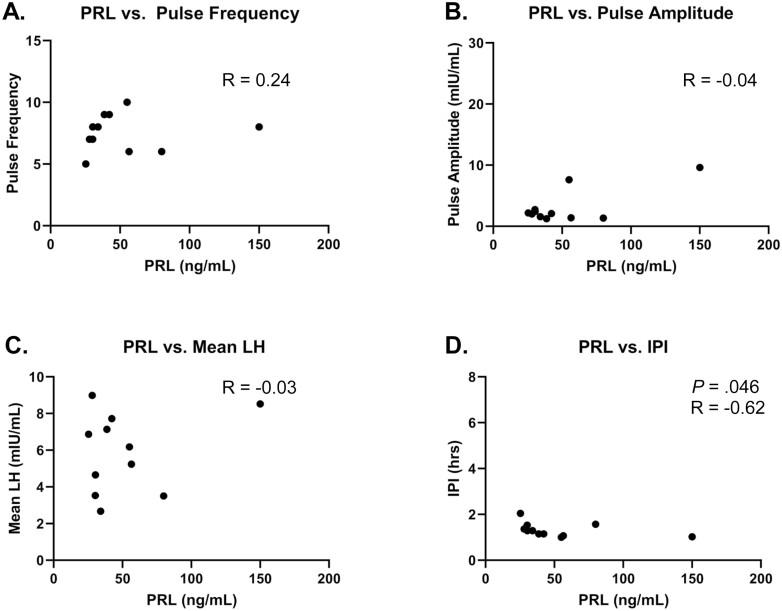
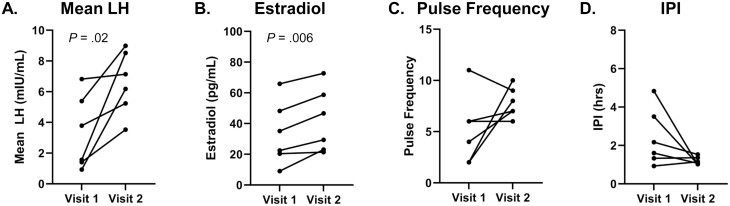
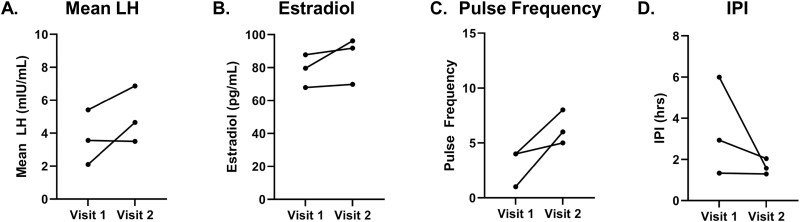
Results: Repetitive intravenous bolus kisspeptin administration increased the total number of LH pulses in the setting of hyperprolactinemia. The interpulse interval declined during the same time frames. LH pulse amplitude did not change, but the mean LH rose. In 6 participants with progesterone levels suggestive of an anovulatory state, mean LH and estradiol levels increased significantly at visit 2. In the entire cohort, follicle-stimulating hormone and prolactin levels did not change significantly across the 2 visits. A total of 73% of subjects exhibited an LH pulse within 30 minutes of first kisspeptin dose.
Conclusion: Kisspeptin is capable of stimulating hypothalamic GnRH-induced LH pulses in the setting of hyperprolactinemia.
Keywords: hyperprolactinemia; kisspeptin.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

References
-
- Vroonen L, Jaffrain-Rea ML, Petrossians P, et al. Prolactinomas resistant to standard doses of cabergoline: a multicenter study of 92 patients. Eur J Endocrinol. 2012;167(5):651-662. - PubMed
-
- Delgrange E, Daems T, Verhelst J, Abs R, Maiter D. Characterization of resistance to the prolactin-lowering effects of cabergoline in macroprolactinomas: a study in 122 patients. Eur J Endocrinol. 2009;160(5):747-752. - PubMed
-
- Vergès B, Boureille F, Goudet P, et al. Pituitary disease in MEN type 1 (MEN1): data from the France-Belgium MEN1 multicenter study. J Clin Endocrinol Metab. 2002;87(2):457-465. - PubMed
-
- Molitch ME. Pharmacologic resistance in prolactinoma patients. Pituitary. 2005;8(1):43-52. - PubMed
-
- Weintraub D, David AS, Evans AH, Grant JE, Stacy M. Clinical spectrum of impulse control disorders in Parkinson’s disease. Mov Disord. 2015;30(2):121-127. - PubMed
