

Provider preferences for delivery of HIV care coordination services: results from a discrete choice experiment
- PMID: 35324055
- PMCID: PMC8944220
- DOI: 10.1002/jia2.25887
Provider preferences for delivery of HIV care coordination services: results from a discrete choice experiment
Abstract
Introduction: The PROMISE study was launched in 2018 to assess and document the implementation of changes to an existing HIV Care Coordination Programme (CCP) designed to address persistent disparities in care and treatment engagement among persons with HIV in New York City. We evaluated provider endorsement of features of the CCP to understand drivers of engagement with the programme.
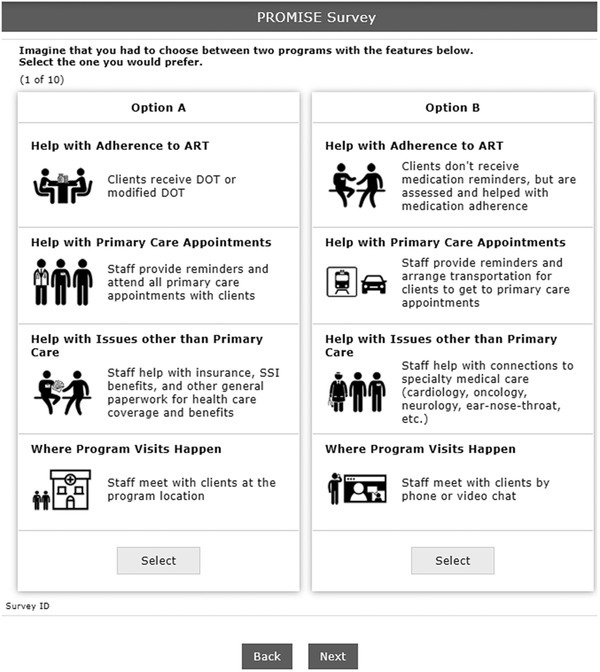
Methods: We used a discrete choice experiment to measure provider endorsement of four CCP attributes, including: (1) how CCP helps with medication adherence, (2) how CCP helps with primary care appointments, (3) how CCP helps with issues other than primary care and (4) where CCP visits take place (visit location). Each attribute had three to four levels. Our primary outcomes were relative importance and part-worth utilities, measures of preference for the levels of the four CCP program attributes, estimated using a hierarchical-Bayesian multinomial logit model. All non-medical providers in the core CCP positions of patient navigator, care coordinator and programme director or other administrator from each of the 25 revised CCP-implementing agencies were eligible to participate.
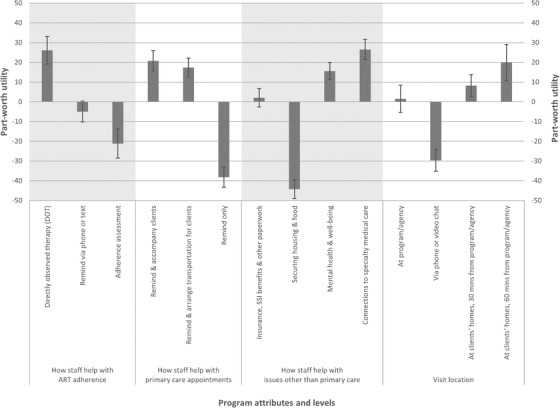
Results: We received responses from 152 providers, 68% of whom identified as women, 49% identified as Latino/a, 34% identified as Black and 60% were 30-49 years old. Visit location (28.6%, 95% confidence interval [CI] 27.0-30.3%) had the highest relative importance, followed by how staff help with ART adherence (24.3%, 95% CI 22.4-26.1%), how staff help with issues other than primary care (24.2%, 95% CI 22.7-25.7%) and how staff help with primary care appointments (22.9%, 95% CI 21.7-24.1%). Within each of the above attributes, respectively, the levels with the highest part-worth utilities were home visits 60 minutes from the program or agency (utility 19.9, 95% CI 10.7-29.0), directly observed therapy (utility 26.1, 95% CI 19.1-33.1), help with non-HIV specialty medical care (utility 26.5, 95% CI 21.5-31.6) and reminding clients about and accompanying them to primary care appointments (utility 20.8, 95% CI 15.6-26.0).
Conclusions: Ongoing CCP refinements should account for how best to support and evaluate the intensive CCP components endorsed by providers in this study.
Keywords: HIV; New York City; adherence; antiretroviral therapy; care coordination; discrete choice experiment.
© 2022 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Conflict of interest statement
There are no competing interests.
Figures
Similar articles
-
Heterogeneity of provider preferences for HIV Care Coordination Program features: latent class analysis of a discrete choice experiment.HIV Res Clin Pract. 2024 Dec 31;25(1):2300923. Epub 2024 Jan 22. HIV Res Clin Pract. 2024. PMID: 38251822
-
Are client and provider preferences for HIV care coordination programme features concordant? Discrete choice experiments in Ryan White part A-funded New York City care coordination programmes.BMJ Open. 2025 Jun 24;15(6):e097918. doi: 10.1136/bmjopen-2024-097918. BMJ Open. 2025. PMID: 40555448 Free PMC article.
-
Client preferences for HIV Care Coordination Program features in New York City: latent class analysis of a discrete choice experiment.J Int AIDS Soc. 2023 Aug;26(8):e26162. doi: 10.1002/jia2.26162. J Int AIDS Soc. 2023. PMID: 37643295 Free PMC article.
-
Exploring Relative Preferences for HIV Service Features Using Discrete Choice Experiments: a Synthetic Review.Curr HIV/AIDS Rep. 2020 Oct;17(5):467-477. doi: 10.1007/s11904-020-00520-3. Curr HIV/AIDS Rep. 2020. PMID: 32860150 Free PMC article. Review.
-
Development of attributes and attribute levels for a discrete choice experiment on patients' and providers' choice for antiretroviral therapy service in Northwest Ethiopia.AIDS Res Ther. 2023 Jun 4;20(1):33. doi: 10.1186/s12981-023-00531-1. AIDS Res Ther. 2023. Retraction in: AIDS Res Ther. 2023 Aug 24;20(1):58. doi: 10.1186/s12981-023-00555-7. PMID: 37271808 Free PMC article. Retracted. Review.
Cited by
-
Heterogeneity of provider preferences for HIV Care Coordination Program features: latent class analysis of a discrete choice experiment.HIV Res Clin Pract. 2024 Dec 31;25(1):2300923. Epub 2024 Jan 22. HIV Res Clin Pract. 2024. PMID: 38251822
-
Are client and provider preferences for HIV care coordination programme features concordant? Discrete choice experiments in Ryan White part A-funded New York City care coordination programmes.BMJ Open. 2025 Jun 24;15(6):e097918. doi: 10.1136/bmjopen-2024-097918. BMJ Open. 2025. PMID: 40555448 Free PMC article.
-
The Evolving Landscape of Discrete Choice Experiments in Health Economics: A Systematic Review.Pharmacoeconomics. 2025 Aug;43(8):879-936. doi: 10.1007/s40273-025-01495-y. Epub 2025 May 21. Pharmacoeconomics. 2025. PMID: 40397369 Free PMC article.
-
Client preferences for HIV Care Coordination Program features in New York City: latent class analysis of a discrete choice experiment.J Int AIDS Soc. 2023 Aug;26(8):e26162. doi: 10.1002/jia2.26162. J Int AIDS Soc. 2023. PMID: 37643295 Free PMC article.
References
-
- Centers for Disease Control and Prevention . Monitoring selected national HIV prevention and care objectives by using HIV surveillance data United States and 6 dependent areas, 2019: national profile. HIV Surveillance Supplemental Report. 2021. [cited 2021 Nov 11]. Available from: https://www.cdc.gov/hiv/library/reports/hiv‐surveillance/vol‐26‐no‐2/con...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
