

Management of Cervical Spondylotic Radiculopathy: A Systematic review
- PMID: 35324370
- PMCID: PMC9609507
- DOI: 10.1177/21925682221075290
Management of Cervical Spondylotic Radiculopathy: A Systematic review
Abstract
Objective: (1) To evaluate the effects of surgery and conservative treatments for cervical spondylotic radiculopathy and (2) provide reference for choosing the time and method of treatment.
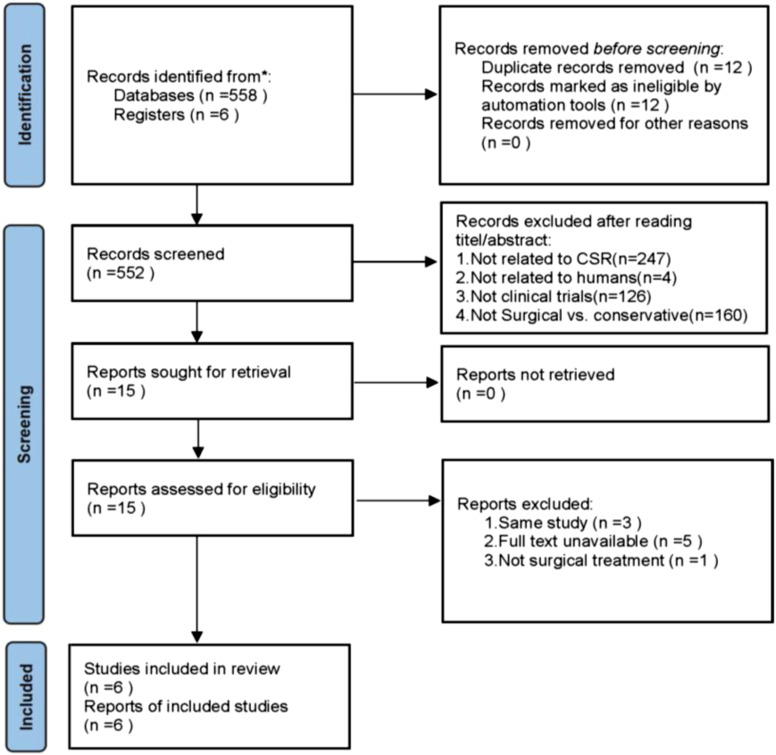
Methods: A literature search was performed using PubMed, EMbase, The Cochrane Library, Web of Science, and ClinicalTrials from inception to September 2021. Randomized controlled trials (RCTs) on the use of surgery or conservative Treatments in Cervical Spondylotic Radiculopathy (CSR) were selected. The primary outcomes were the neck and arm visual analog scale (VAS) and Neck Disability Index (NDI). Secondary outcomes included active range of cervical motion (ROM) and Mental Health. Two reviewers proceeded study selection and quality assessment.
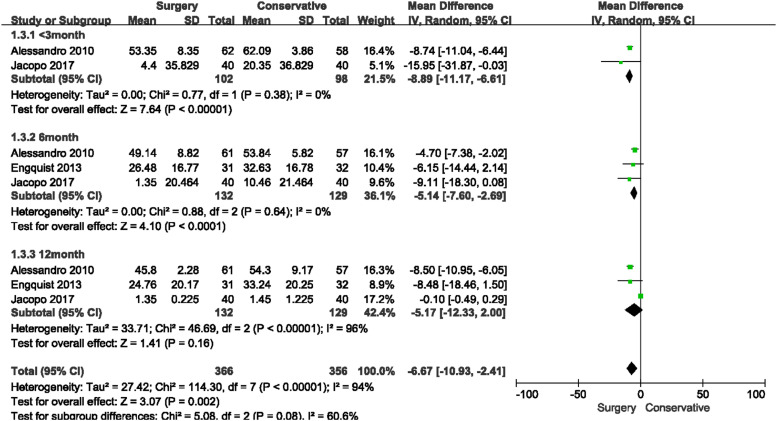
Results: A total of 6 studies, which comprised a total of 464 participants were included in the final meta-analysis. Compared with conservative treatment, surgical treatment was more effective in lowering Neck-VAS (<3 m: MD = -29.44, 95% CI = (-41.62,-17.27), P < .00001; 3-6 M: MD = -20.97, 95% CI = (-26.36,-15.57), P < .00001; 6 M: MD = -13.40, 95% CI = (-19.39, -7.41), P<.0001; 12 M: MD=-15.53, 95% CI=(-28.38, -2.68), P=.02), Arm-VAS(<3 m: MD = -33.52, 95% CI = (-39.89, -27.16), P < .00001; 3-6 M: MD = -20.97, 95% CI = (-26.36, -15.57), P < .00001; 6 M: MD = -17.52, 95% CI=(-23.94, -11.11), P < .0001; 12 M: MD = -21.91, 95% CI=(-27.09, -16.72), P < .00001) and NDI (<3 m: MD = -8.89, 95% CI = (-11.17, -6.61), P < .00001; 6 M: MD = -5.14, 95% CI = (-7.60, -2.69), P < .0001). No significant difference was observed in NDI at 12-month time point (MD = -5.17, 95% CI = (-12.33, 2.00), P = .16), ROM(MD = 2.91, 95% CI = (-4.51, 10.33), P = .77) and Mental Health (MD = .05, 95% CI=(-.24, .33), P = .74).
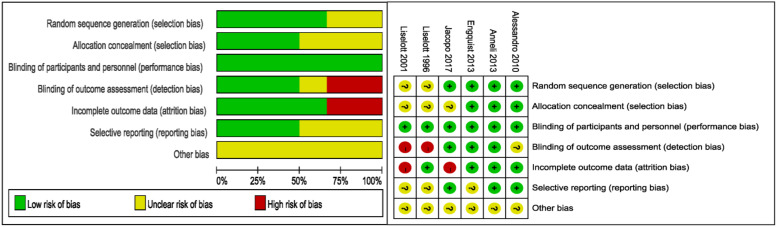
Conclusion: The 6 included studies that had low risk of bias, providing high-quality evidence for the surgical efficacy of CSR. The evidence indicates that surgical treatment is better than conservative treatment in terms of VAS score and NDI score, and superior to conservative treatment in less than one year. There was no evidence of a difference between surgical and conservative care in ROM and mental health. A small sample study with a follow-up of 5 to 8 years showed that surgical treatment was still better than conservative treatment, but the sample size was small and the results should be carefully interpreted.Compared with conservative treatment, surgical treatment had a faster onset of response, especially in pain relief, but did not have a significant advantage in range of motion or NDI. This seems to mean that for patients with severe or even unbearable pain, the benefits of surgery as soon as possible will be significant. Although it is not clear whether the short-term risks of surgery are outweighed by the long-term benefits, rapid pain relief is necessary. Conservative treatment (including medical exercise therapy, mechanical cervical tractions, transcutaneous electrical nerve stimulation, pain management education, and cervical collar) once or twice a week for 3 months is beneficial in the long term and avoids the risks of surgery. In consideration of the good natural history of CSR and the relatively good outcome of conservative treatment (although symptom relief is slow), we think that surgery is not necessary for patients who do not need rapid pain relief.
Keywords: Cervical Spondylotic Radiculopathy; Conservative Treatments; Surgery; Systematic review.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures




Similar articles
-
Comparison of clinical outcomes and complications of biportal and uniportal endoscopic decompression for the treatment of cervical spondylotic radiculopathy: A systematic review and meta-analysis.Jt Dis Relat Surg. 2024 Aug 14;35(3):583-593. doi: 10.52312/jdrs.2024.1820. Epub 2024 Aug 14. Jt Dis Relat Surg. 2024. PMID: 39189567 Free PMC article.
-
Efficacy and Safety of Acupuncture in the Treatment of Radicular Cervical Spondylosis: A Systematic Review and Meta-Analysis.Comb Chem High Throughput Screen. 2024;27(19):2951-2962. doi: 10.2174/0113862073265007231108050338. Comb Chem High Throughput Screen. 2024. PMID: 37957858 Free PMC article.
-
Predictive Effect of Cervical Sagittal Parameters on Conservative Treatment of Single-Segment Cervical Spondylotic Radiculopathy.World Neurosurg. 2020 Feb;134:e1028-e1036. doi: 10.1016/j.wneu.2019.11.081. Epub 2019 Nov 20. World Neurosurg. 2020. PMID: 31759147
-
Arthroplasty for cervical spondylotic myelopathy: similar results to patients with only radiculopathy at 3 years' follow-up.J Neurosurg Spine. 2014 Sep;21(3):400-10. doi: 10.3171/2014.3.SPINE13387. Epub 2014 Jun 13. J Neurosurg Spine. 2014. PMID: 24926929
-
Minimally Invasive Full-Endoscopic Posterior Cervical Foraminotomy Assisted by O-Arm-Based Navigation.Pain Physician. 2018 May;21(3):E215-E223. Pain Physician. 2018. PMID: 29871377
Cited by
-
Improvement in Chronic Low Back and Intermittent Chronic Neck Pain, Disability, and Improved Spine Parameters Using Chiropractic BioPhysics® Rehabilitation After 5 Years of Failed Chiropractic Manipulation: A Case Report and 1-Year Follow-Up.Healthcare (Basel). 2025 Apr 3;13(7):814. doi: 10.3390/healthcare13070814. Healthcare (Basel). 2025. PMID: 40218115 Free PMC article.
-
The Efficacy of Cervical Lordosis Rehabilitation for Nerve Root Function and Pain in Cervical Spondylotic Radiculopathy: A Randomized Trial with 2-Year Follow-Up.J Clin Med. 2022 Nov 2;11(21):6515. doi: 10.3390/jcm11216515. J Clin Med. 2022. PMID: 36362743 Free PMC article.
-
Investigating the brain functional abnormalities underlying pain hypervigilance in chronic neck and shoulder pain: a resting-state fMRI study.Neuroradiology. 2024 Aug;66(8):1353-1361. doi: 10.1007/s00234-024-03286-2. Epub 2024 Feb 1. Neuroradiology. 2024. PMID: 38296904
-
The effects of modified Guizhi plus Gegen decoction combined with the blade needle therapy on TCM syndromes, cervical curvature and levels of inflammatory factors in patients with cervical spondylotic radiculopathy.Am J Transl Res. 2023 Aug 15;15(8):5347-5355. eCollection 2023. Am J Transl Res. 2023. PMID: 37692957 Free PMC article.
-
Cervical Radiculopathy as a Hidden Cause of Angina: Cervicogenic Angina.J Med Cases. 2022 Nov;13(11):545-550. doi: 10.14740/jmc4025. Epub 2022 Nov 27. J Med Cases. 2022. PMID: 36506762 Free PMC article.
References
-
- Zhu LG, Yu J. Research progress of non-operative treatment for cervical spondylotic radiculopathy. Chin J Trad Med Traum Orthop. 2011; 19(4): 66-69.
-
- Wang YG, Guo XQ, Zhang Q, et al. A systematic review on the treatment of nerve root cervical disease by manipulation. Chin J Trad Chin Med Phar. 2013; 28(2): 499-503.
-
- Zhu GM, Sun WQ, Shen GQ, et al. Mechanisms of spinal micro-adjustment manipulations in treating cervical spondylotic radiculopathy. J Acupuncture Chiropractic Tuina Sci. 2007; 5: 68-70.
-
- Mayfield FH. Cervical spondylotic and myelopathy. Adv Neurol. 1985; 22: 307-321. - PubMed
-
- Epstein JA, Lavine LS, Aronson HA, Epstein BS. Cervical spondylotic radiculopathy. Clin Orthop Relat Res. 1965; 40: 113-122. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
