

Prevention of violence against women and girls: A cost-effectiveness study across 6 low- and middle-income countries
- PMID: 35324910
- PMCID: PMC8946747
- DOI: 10.1371/journal.pmed.1003827
Prevention of violence against women and girls: A cost-effectiveness study across 6 low- and middle-income countries
Abstract
Background: Violence against women and girls (VAWG) is a human rights violation with social, economic, and health consequences for survivors, perpetrators, and society. Robust evidence on economic, social, and health impact, plus the cost of delivery of VAWG prevention, is critical to making the case for investment, particularly in low- and middle-income countries (LMICs) where health sector resources are highly constrained. We report on the costs and health impact of VAWG prevention in 6 countries.
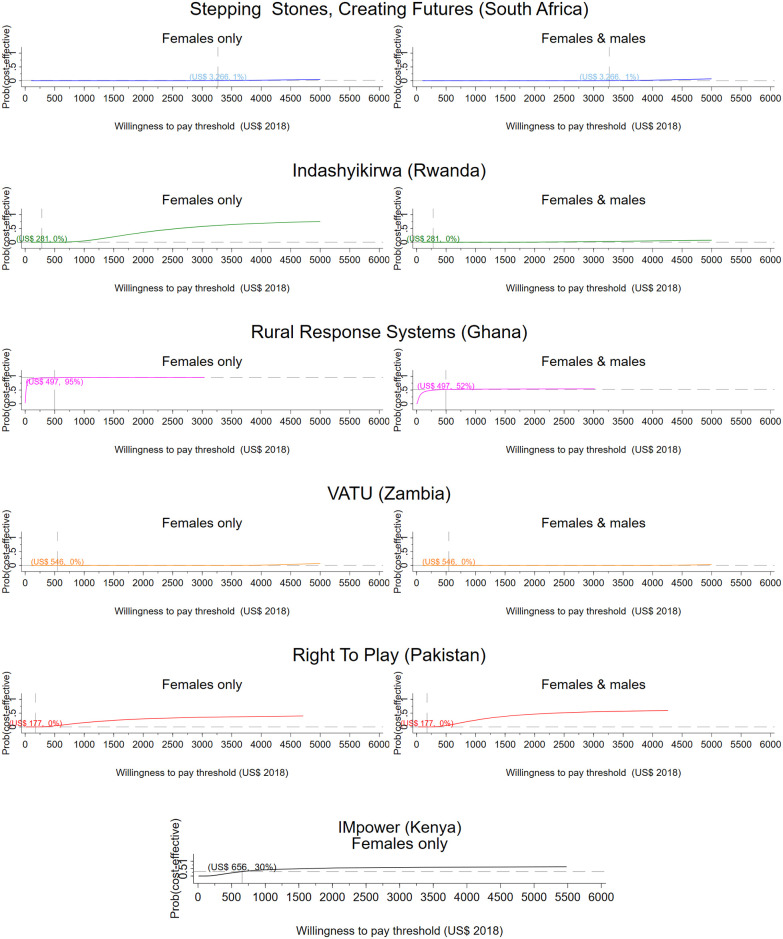
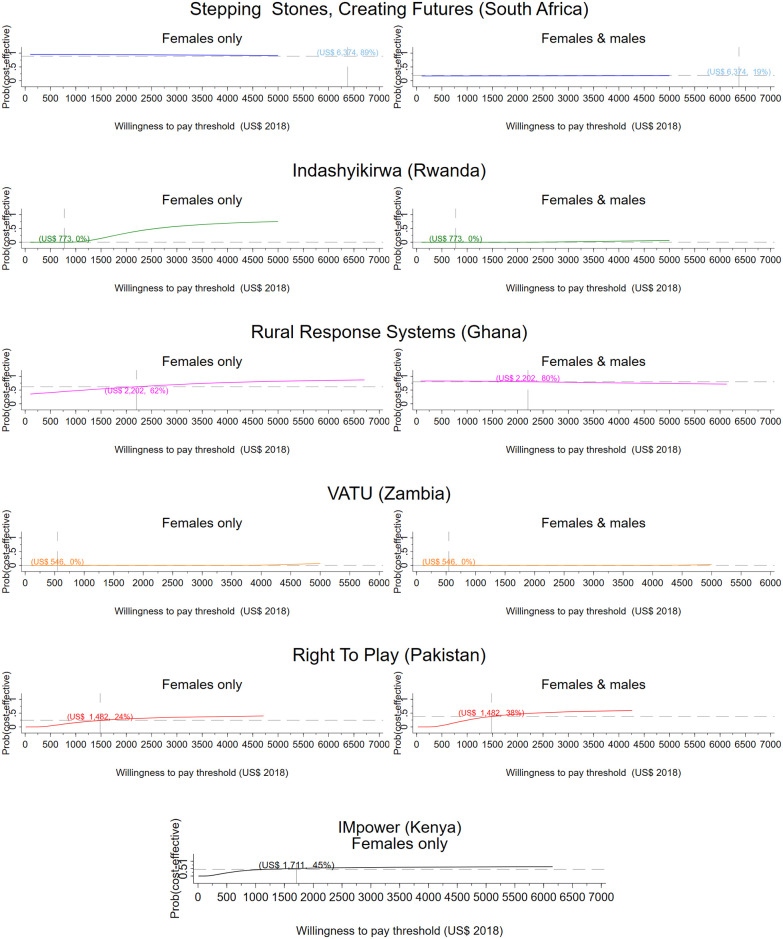
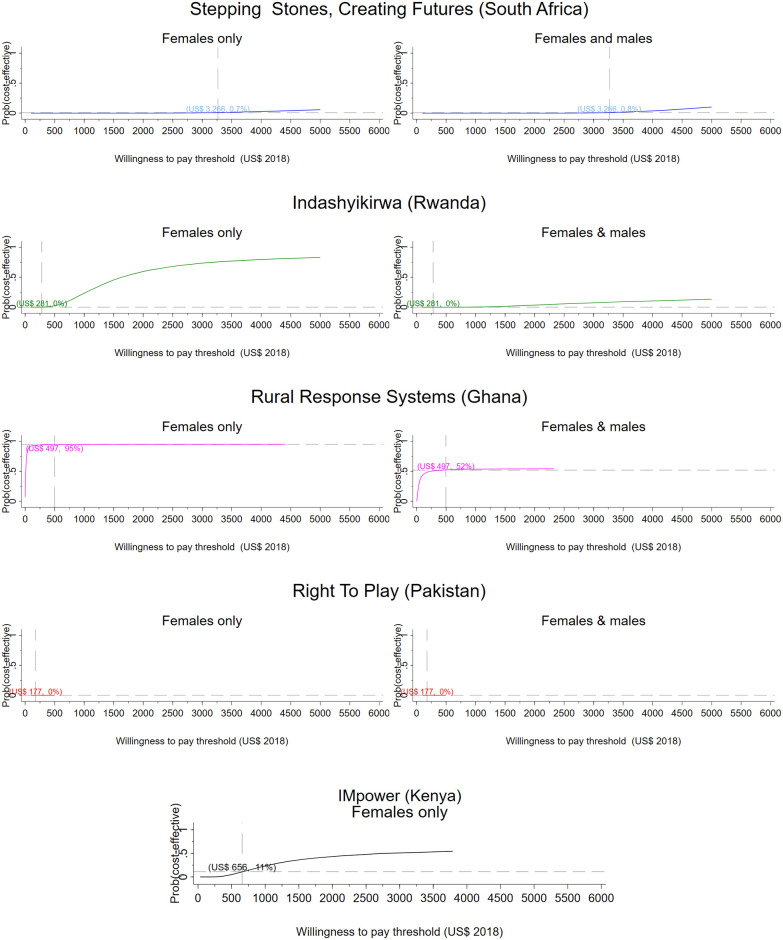
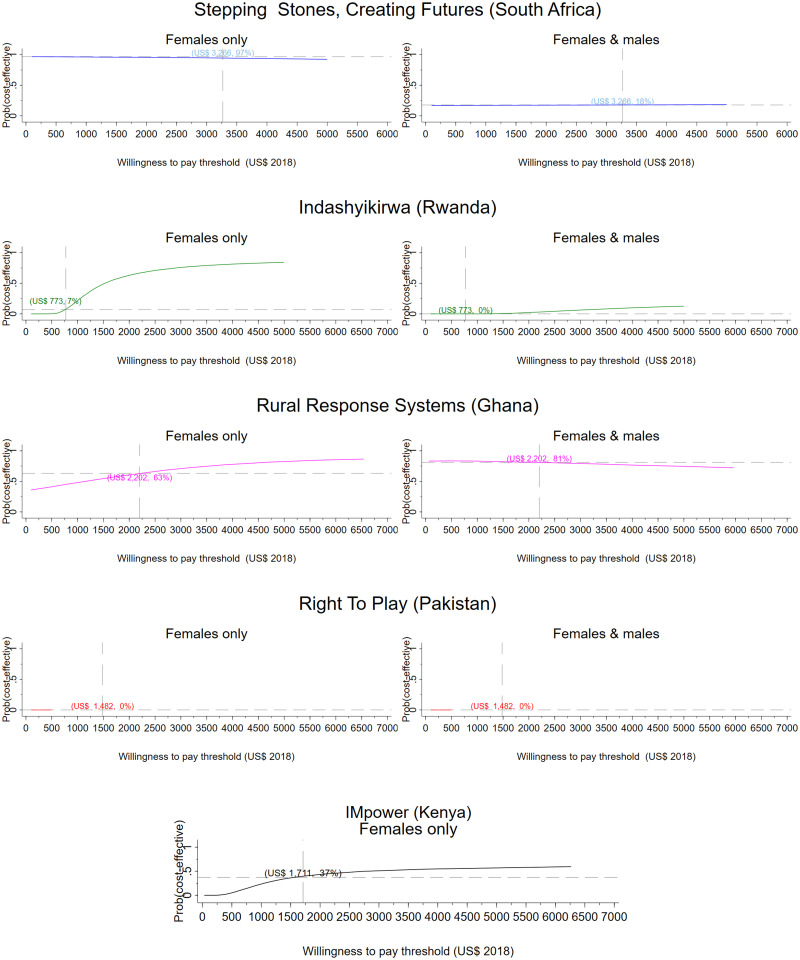
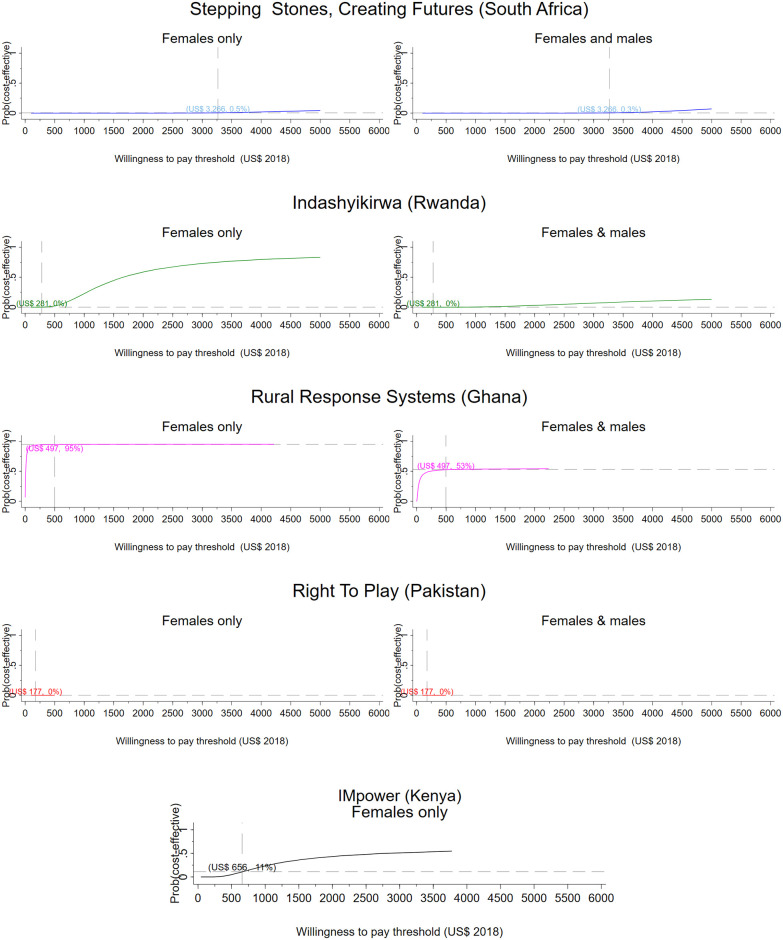
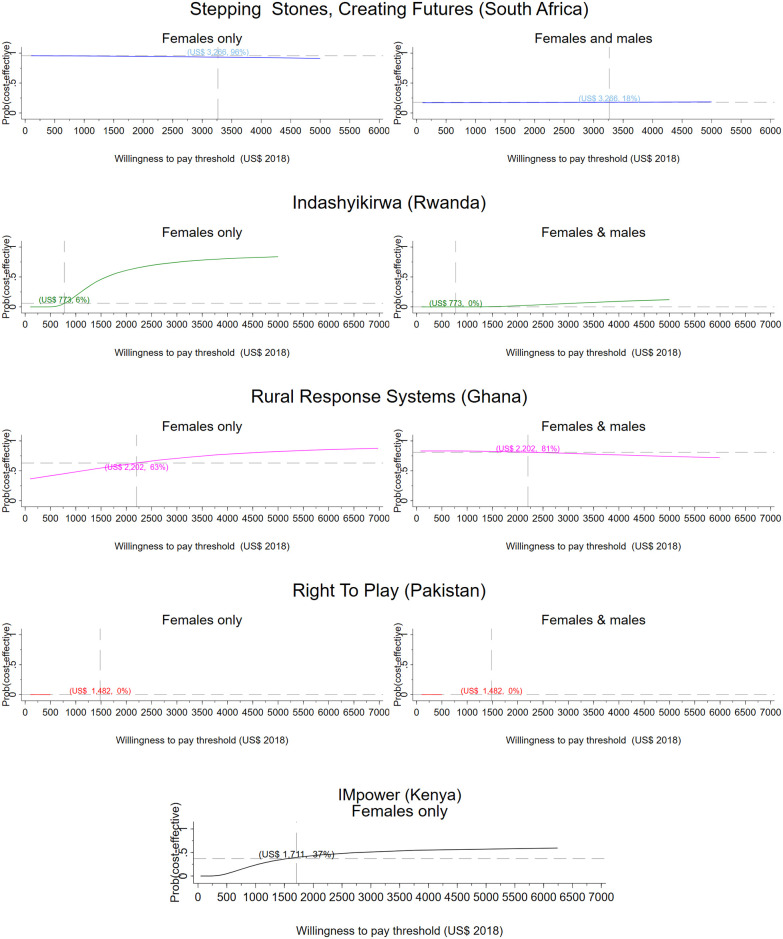
Methods and findings: We conducted a trial-based cost-effectiveness analysis of VAWG prevention interventions using primary data from 5 randomised controlled trials (RCTs) in sub-Saharan Africa and 1 in South Asia. We evaluated 2 school-based interventions aimed at adolescents (11 to 14 years old) and 2 workshop-based (small group or one to one) interventions, 1 community-based intervention, and 1 combined small group and community-based programme all aimed at adult men and women (18+ years old). All interventions were delivered between 2015 and 2018 and were compared to a do-nothing scenario, except for one of the school-based interventions (government-mandated programme) and for the combined intervention (access to financial services in small groups). We computed the health burden from VAWG with disability-adjusted life year (DALY). We estimated per capita DALYs averted using statistical models that reflect each trial's design and any baseline imbalances. We report cost-effectiveness as cost per DALY averted and characterise uncertainty in the estimates with probabilistic sensitivity analysis (PSA) and cost-effectiveness acceptability curves (CEACs), which show the probability of cost-effectiveness at different thresholds. We report a subgroup analysis of the small group component of the combined intervention and no other subgroup analysis. We also report an impact inventory to illustrate interventions' socioeconomic impact beyond health. We use a 3% discount rate for investment costs and a 1-year time horizon, assuming no effects post the intervention period. From a health sector perspective, the cost per DALY averted varies between US$222 (2018), for an established gender attitudes and harmful social norms change community-based intervention in Ghana, to US$17,548 (2018) for a livelihoods intervention in South Africa. Taking a societal perspective and including wider economic impact improves the cost-effectiveness of some interventions but reduces others. For example, interventions with positive economic impacts, often those with explicit economic goals, offset implementation costs and achieve more favourable cost-effectiveness ratios. Results are robust to sensitivity analyses. Our DALYs include a subset of the health consequences of VAWG exposure; we assume no mortality impact from any of the health consequences included in the DALYs calculations. In both cases, we may be underestimating overall health impact. We also do not report on participants' health costs.
Conclusions: We demonstrate that investment in established community-based VAWG prevention interventions can improve population health in LMICs, even within highly constrained health budgets. However, several VAWG prevention interventions require further modification to achieve affordability and cost-effectiveness at scale. Broadening the range of social, health, and economic outcomes captured in future cost-effectiveness assessments remains critical to justifying the investment urgently required to prevent VAWG globally.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: CW was the Chief Scientific Adviser at the Department for International Development (UKAid) at the time of writing. This work was conducted as part of her academic role as professor in epidemiology at the London School of Hygiene & Tropical Medicine.
Figures
References
-
- Creditor Reporting System (CRS). [cited 2020 Mar 26]. https://stats.oecd.org/Index.aspx?DataSetCode=CRS1#.
-
- What Works. What Works—What Works to Prevent VAWG: Research and Innovation Programme—Final Performance Evaluation. 2020 [cited 2020 Jul 27]. https://www.whatworks.co.za/resources/reports/item/716-what-works-to-pre....
-
- Abramsky T, Devries K, Kiss L, Nakuti J, Kyegombe N, Starmann E, et al.. Findings from the SASA! Study: a cluster randomized controlled trial to assess the impact of a community mobilization intervention to prevent violence against women and reduce HIV risk in Kampala. Uganda BMC Med. 2014;12:122. doi: 10.1186/s12916-014-0122-5 - DOI - PMC - PubMed
-
- Ogum Alangea D, Addo-Lartey AA, Chirwa ED, Sikweyiya Y, Coker-Appiah D, Jewkes R, et al.. Evaluation of the rural response system intervention to prevent violence against women: findings from a community-randomised controlled trial in the Central Region of Ghana. Glob Health Action. 2020;13:1711336. doi: 10.1080/16549716.2019.1711336 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
