

Age-Specific Prevalence of Anal and Cervical Human Papillomavirus Infection and High-Grade Lesions in 11 177 Women by Human Immunodeficiency Virus Status: A Collaborative Pooled Analysis of 26 Studies
- PMID: 35325151
- PMCID: PMC10152502
- DOI: 10.1093/infdis/jiac108
Age-Specific Prevalence of Anal and Cervical Human Papillomavirus Infection and High-Grade Lesions in 11 177 Women by Human Immunodeficiency Virus Status: A Collaborative Pooled Analysis of 26 Studies
Abstract
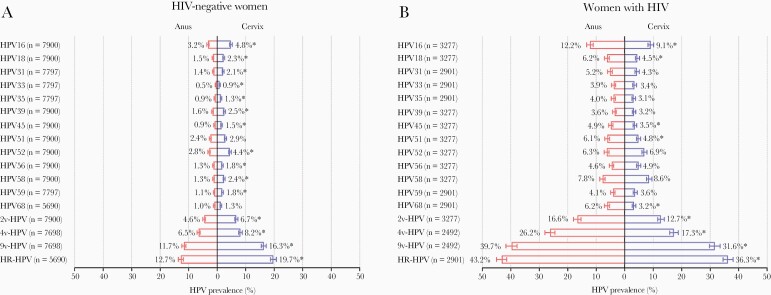
Background: Age-specific data on anal, and corresponding cervical, human papillomavirus (HPV) infection are needed to inform female anal cancer prevention.
Methods: We centrally reanalyzed individual-level data from 26 studies reporting HPV prevalence in paired anal and cervical samples by human immunodeficiency virus (HIV) status and age. For women with HIV (WWH) with anal high-grade squamous intraepithelial lesions or worse (HSIL+), we also investigated concurrent cervical cytopathology.
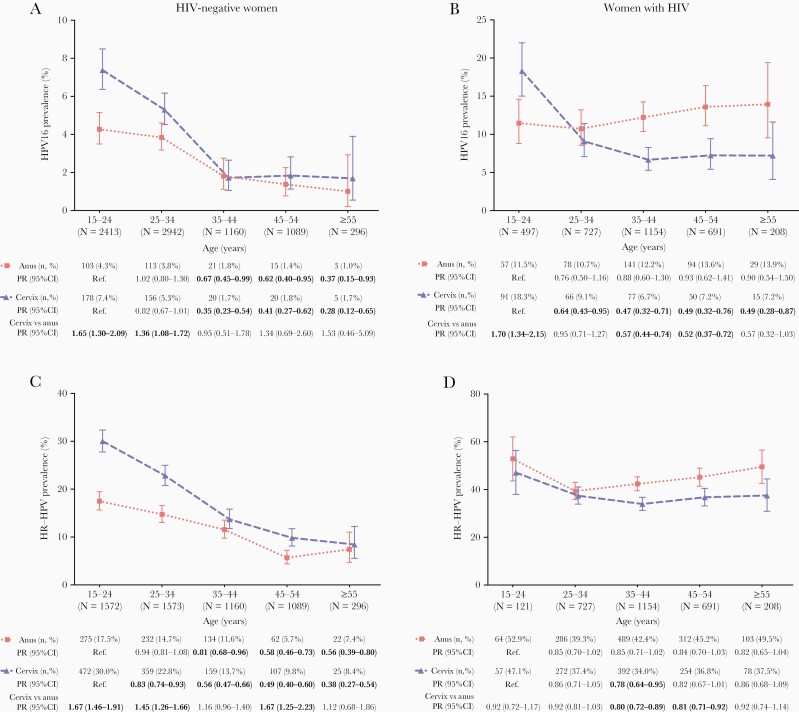
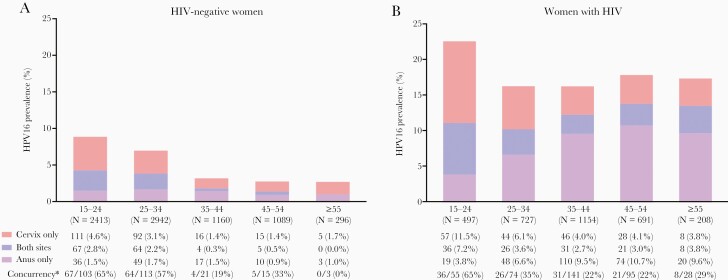
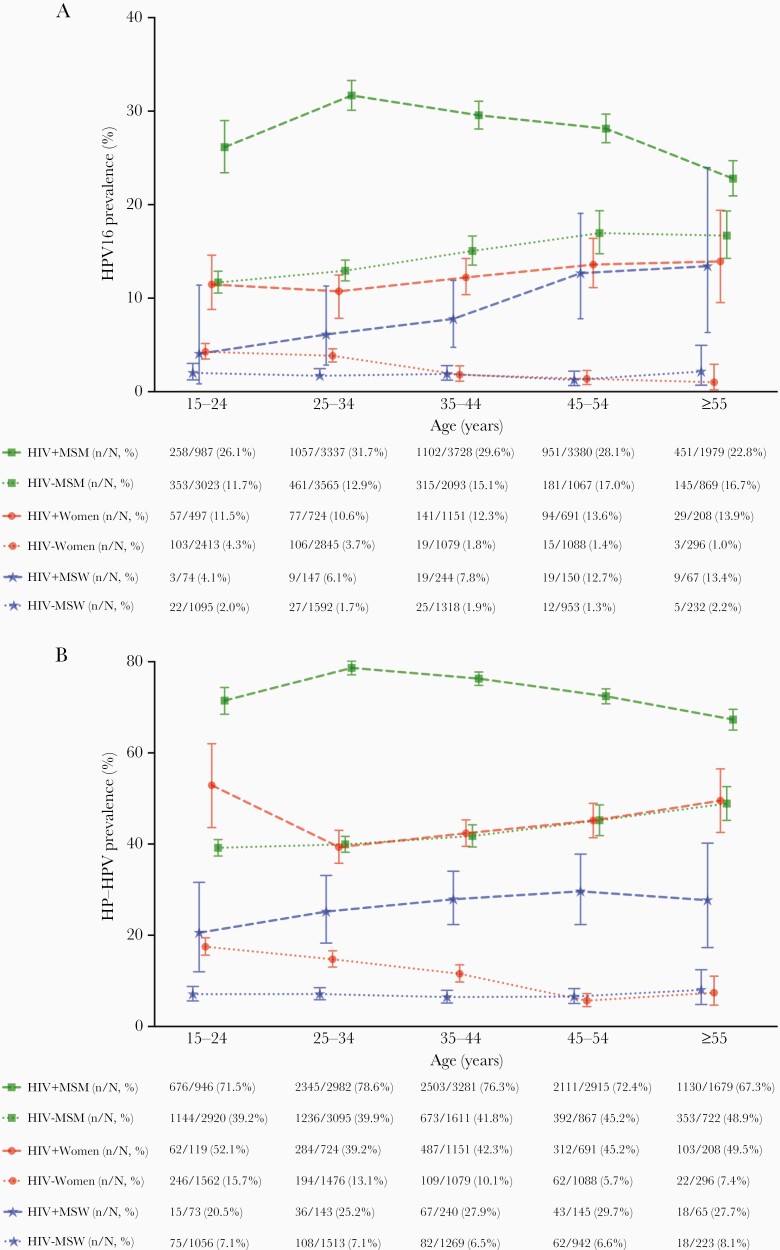
Results: In HIV-negative women, HPV16 prevalence decreased significantly with age, both at anus (4.3% at 15-24 years to 1.0% at ≥55 years; ptrend = 0.0026) and cervix (7.4% to 1.7%; ptrend < 0.0001). In WWH, HPV16 prevalence decreased with age at cervix (18.3% to 7.2%; ptrend = 0.0035) but not anus (11.5% to 13.9%; ptrend = 0.5412). Given anal HPV16 positivity, concurrent cervical HPV16 positivity also decreased with age, both in HIV-negative women (ptrend = 0.0005) and WWH (ptrend = 0.0166). Among 48 WWH with HPV16-positive anal HSIL+, 27 (56%) were cervical high-risk HPV-positive, including 8 with cervical HPV16, and 5 were cervical HSIL+.
Conclusions: Age-specific shifts in HPV16 prevalence from cervix to anus suggest that HPV infections in the anus persist longer, or occur later in life, than in the cervix, particularly in WWH. This is an important consideration when assessing the utility of cervical screening results to stratify anal cancer risk.
Keywords: HIV; HPV; anus; cervix; women.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. A. P. O. reports grants made to her institutions from AMC, grant no. 2UM1CA121947 and an UPR/MDACC Partnership grant no. 2U54CA096297 for time and effort support to the present manuscript. She reports NIH grants not related to the current work. She reports consulting fees and payment for lectures from Merck and Co. R. K. was supported by the Canadian Institutes of Health Research (CIHR) for the present manuscript. A. d. P. shared data from the EVVA study for this manuscript. The EVVA study was supported by the CIHR, and the AIDS and Infectious Diseases Network of Fonds de Recherche du Quebec Sante. Payments were made to A. d. P.’s institution. J. M. P. reports grants and personal fees from Merck and Co.; consulting fees from Vir Biotechnology, Antiva Biosciences, and Virion Therapeutics; personal fees Janssen Pharmaceuticals; stock or stock options from Virion Therapeutics and Vir Biotechnology (outside the submitted work); and a leadership role in the International Papillomavirus Society. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Moscicki AB, Schiffman M, Kjaer S, Villa LL. Chapter 5: Updating the natural history of HPV and anogenital cancer. Vaccine 2006; 24 (Suppl 3):S3/42–51. - PubMed
-
- Islami F, Ferlay J, Lortet-Tieulent J, Bray F, Jemal A.. International trends in anal cancer incidence rates. Int J Epidemiol 2017; 46:924–38. - PubMed
-
- de Martel C, Georges D, Bray F, Ferlay J, Clifford GM.. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health 2020; 8:e180–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
