

Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial
- PMID: 35326183
- PMCID: PMC8944471
- DOI: 10.3390/antiox11030533
Outpatient Oral Neuropathic Pain Management with Photobiomodulation Therapy: A Prospective Analgesic Pharmacotherapy-Paralleled Feasibility Trial
Abstract
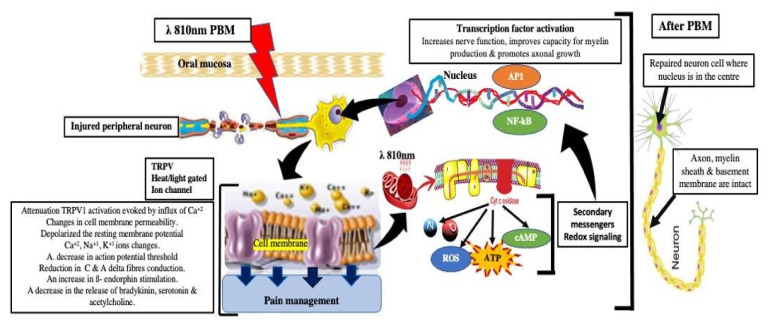
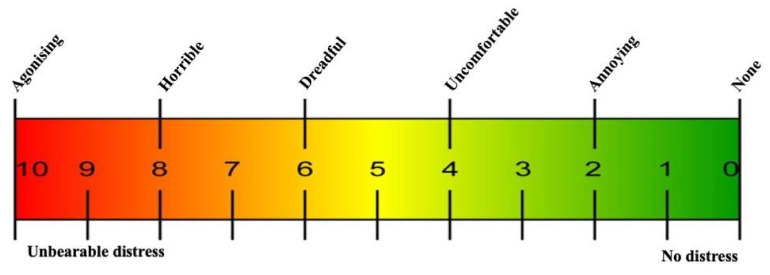
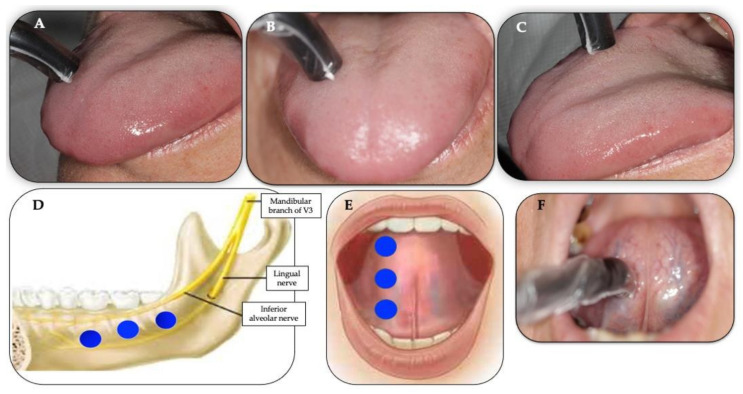
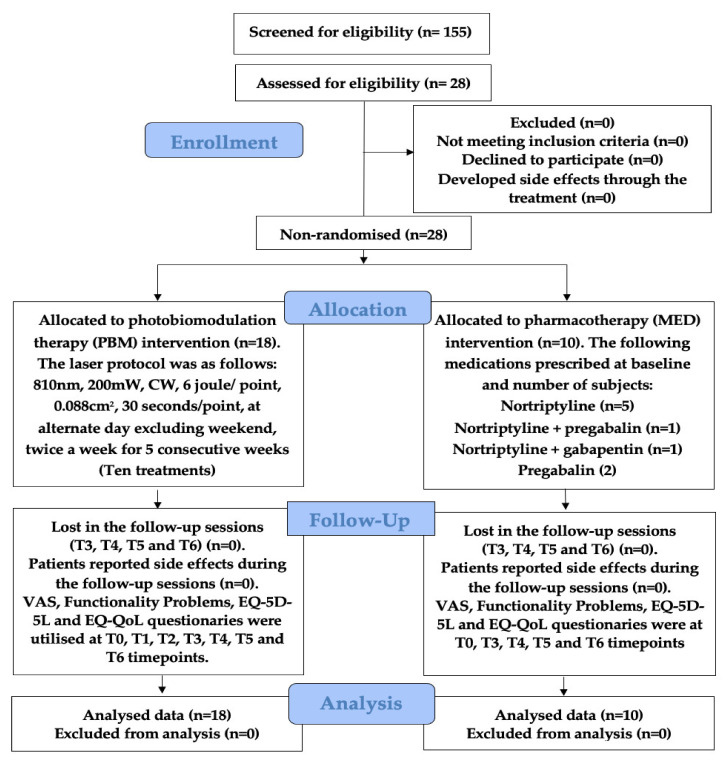
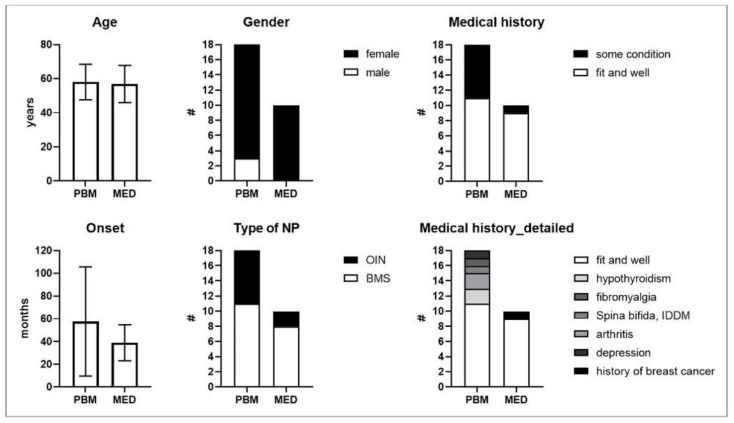
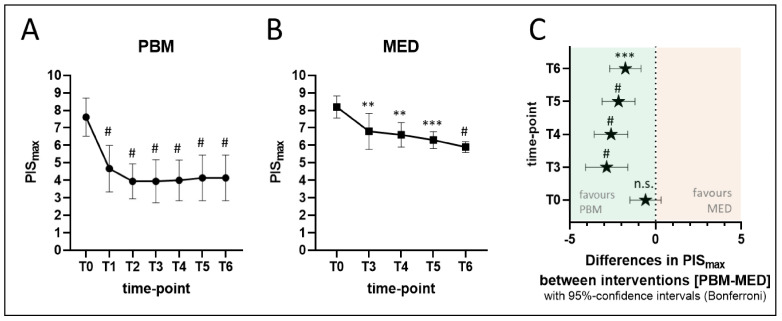
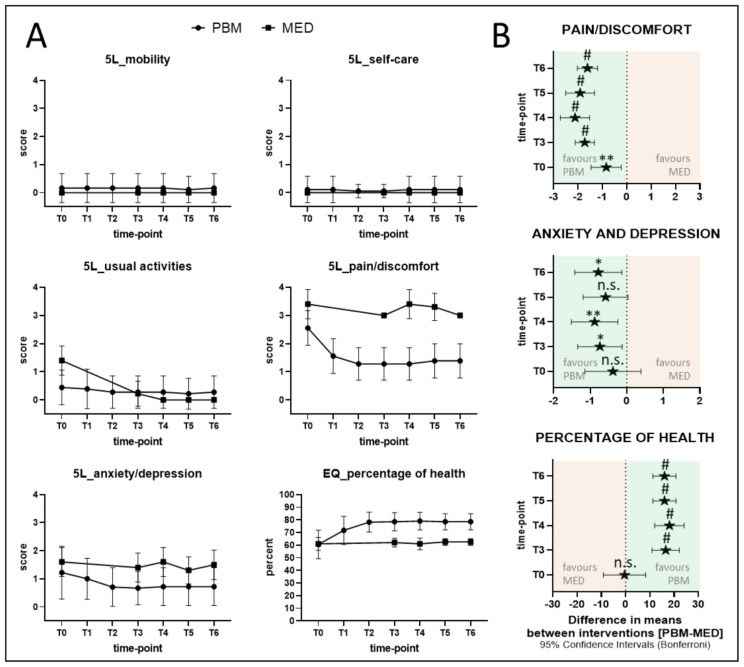
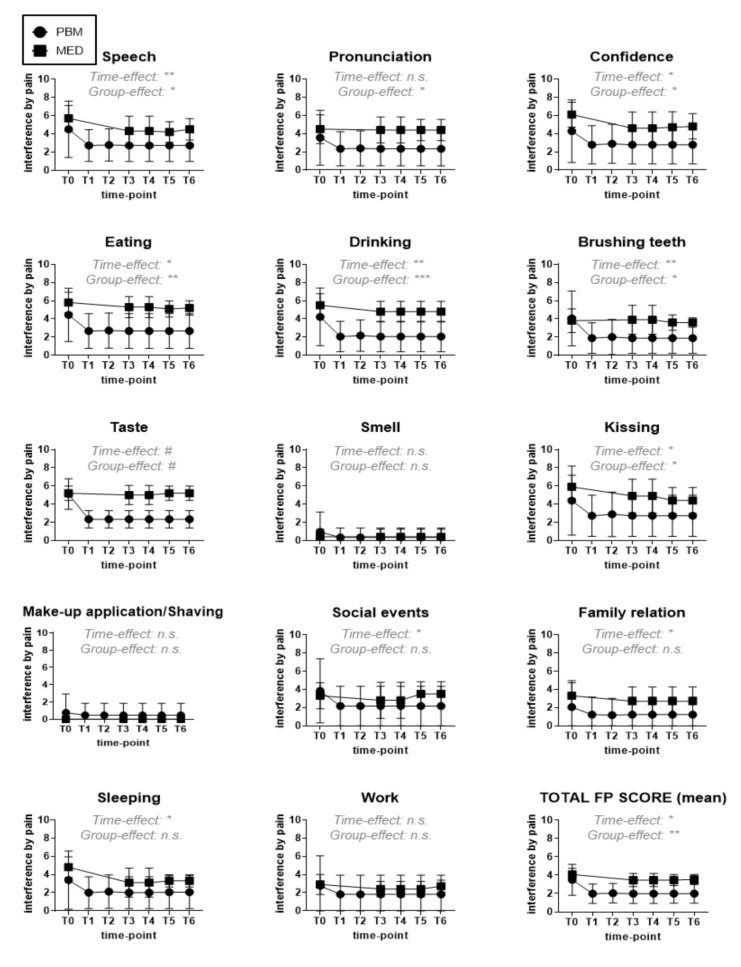
Neuropathic pain (NP) can be challenging to treat effectively as analgesic pharmacotherapy (MED) can reduce pain, but the majority of patients do not experience complete pain relief. Our pilot approach is to assess the feasibility and efficacy of an evidence-based photobiomodulation (PBM) intervention protocol. This would be as an alternative to paralleled standard analgesic MED for modulating NP intensity-related physical function and quality of life (QoL) prospectively in a mixed neurological primary burning mouth syndrome and oral iatrogenic neuropathy study population (n = 28). The study group assignments and outcome evaluation strategy/location depended on the individual patient preferences and convenience rather than on randomisation. Our prospective parallel study aimed to evaluate the possible pre/post-benefit of PBM and to allow for a first qualitative comparison with MED, various patient-reported outcome measures (PROMs) based on Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT-II) were used for up to a nine-month follow-up period in both intervention groups (PBM and MED). The PBM protocol applied to the PBM group was as follows: λ810 nm, 200 mW, 0.088 cm2, 30 s/point, 9 trigger and affected points, twice a week for five consecutive weeks, whereas the MED protocol followed the National Institute of Clinical Excellence (NICE) guidelines. Our results showed that despite the severe and persistent nature of the symptoms of 57.50 ± 47.93 months at baseline in the PBM group, a notably rapid reduction in PISmax on VAS from 7.6 at baseline (T0) to 3.9 at one-month post-treatment (T3) could be achieved. On the other hand, mean PISmax was only reduced from 8.2 at baseline to 6.8 at T3 in the MED group. Our positive PBM findings furthermore support more patients' benefits in improving QoL and functional activities, which were considerably impaired by NP such as: eating, drinking and tasting, whereas the analgesic medication regimens did not. No adverse events were observed in both groups. To the best knowledge of the authors, our study is the first to investigate PBM efficacy as a monotherapy compared to the gold standard analgesic pharmacotherapy. Our positive data proves statistically significant improvements in patient self-reported NP, functionality, psychological profile and QoL at mid- and end-treatment, as well as throughout the follow-up time points (one, three, six and nine months) and sustained up to nine months in the PBM group, compared to the MED group. Our study, for the first time, proves the efficacy and safety of PBM as a potent analgesic in oral NP and as a valid alternative to the gold standard pharmacotherapy approach. Furthermore, we observed long-term pain relief and functional benefits that indicate that PBM modulates NP pathology in a pro-regenerative manner, presumably via antioxidant mechanisms.
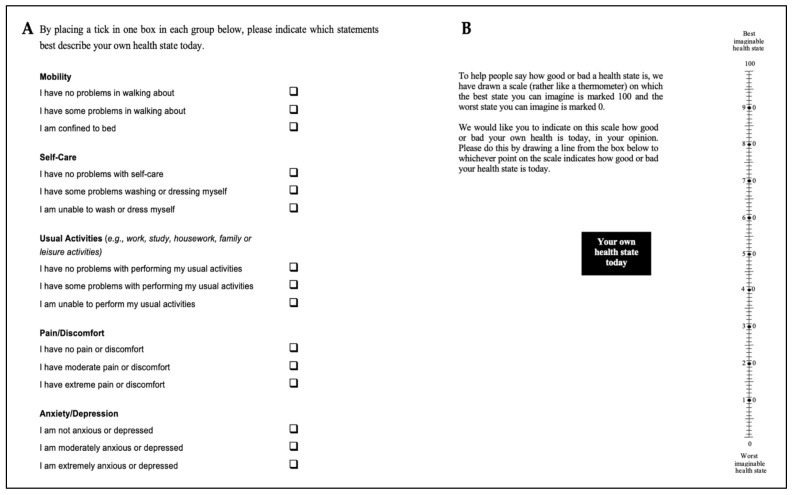
Keywords: EQ-5D-5L; IMMPACT; PROMs; burning mouth syndrome; functional problems; neuropathic pain; oral iatrogenic neuropathy; pharmacotherapy; photobiomodulation therapy; psychological dysfunction; standard analgesic.
Conflict of interest statement
All the authors, including S.V.B. (senior project manager, bredent medical GmbH & Co. KG), J.C. (CEO, Thor Photomedicine Ltd.), P.B. (senior researcher at Thor Photomedicine Ltd.) have declared no conflict of interest.
Figures
Similar articles
-
A Novel Therapeutic Approach of 980 nm Photobiomodulation Delivered with Flattop Beam Profile in Management of Recurrent Aphthous Stomatitis in Paediatrics and Adolescents-A Case Series with 3-Month Follow-Up.J Clin Med. 2024 Mar 29;13(7):2007. doi: 10.3390/jcm13072007. J Clin Med. 2024. PMID: 38610772 Free PMC article.
-
Efficacy and safety of photobiomodulation combined with oral cryotherapy on oral mucosa pain in patients with burning mouth syndrome: a multi-institutional, randomized, controlled trial.BMC Med. 2025 Apr 7;23(1):196. doi: 10.1186/s12916-025-04015-z. BMC Med. 2025. PMID: 40189502 Free PMC article. Clinical Trial.
-
Efficacy of 1064 nm Photobiomodulation Dosimetry Delivered with a Collimated Flat-Top Handpiece in the Management of Peripheral Facial Paralysis in Patients Unresponsive to Standard Treatment Care: A Case Series.J Clin Med. 2023 Sep 29;12(19):6294. doi: 10.3390/jcm12196294. J Clin Med. 2023. PMID: 37834941 Free PMC article.
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
-
Therapeutic Outcomes of Photobiomodulation in Cancer Treatment-induced Oral Mucositis: A Systematic Review.J Clin Exp Dent. 2023 Sep 1;15(9):e749-e759. doi: 10.4317/jced.60710. eCollection 2023 Sep. J Clin Exp Dent. 2023. PMID: 37799759 Free PMC article. Review.
Cited by
-
Effect of Laser Photobiomodulation on Postoperative Pain After Single-Visit Endodontic Treatment in Children: A Randomized Control Trial.Children (Basel). 2024 Dec 12;11(12):1511. doi: 10.3390/children11121511. Children (Basel). 2024. PMID: 39767940 Free PMC article.
-
The Efficacy of Multiwavelength Red and Near-Infrared Transdermal Photobiomodulation Light Therapy in Enhancing Female Fertility Outcomes and Improving Reproductive Health: A Prospective Case Series with 9-Month Follow-Up.J Clin Med. 2024 Nov 24;13(23):7101. doi: 10.3390/jcm13237101. J Clin Med. 2024. PMID: 39685560 Free PMC article.
-
Evaluation of Thyroid Volume Normalisation in Female Patients with Hashimoto Thyroiditis: A 12-Month Comparative Study of Combined Supplements and Photobiomodulation Versus Supplementation Alone.Biomedicines. 2025 Jun 25;13(7):1555. doi: 10.3390/biomedicines13071555. Biomedicines. 2025. PMID: 40722630 Free PMC article.
-
10,600 nm High Level-Laser Therapy Dosimetry in Management of Unresponsive Persistent Peripheral Giant Cell Granuloma to Standard Surgical Approach: A Case Report with 6-Month Follow-Up.J Pers Med. 2023 Dec 25;14(1):26. doi: 10.3390/jpm14010026. J Pers Med. 2023. PMID: 38248727 Free PMC article.
-
[My tongue is burning!-Glossodynia/orofacial pain disorder].Dermatologie (Heidelb). 2022 Sep;73(9):701-707. doi: 10.1007/s00105-022-05037-x. Epub 2022 Aug 23. Dermatologie (Heidelb). 2022. PMID: 35997968 Free PMC article. German.
References
-
- Bennett G.J. Neuropathic pain in the orofacial region: Clinical and research challenges. J. Orofac. Pain. 2004;18:281–286. - PubMed
-
- Bouhassira D., Attal N., Alchaar H., Boureau F., Brochet B., Bruxelle J., Cunin G., Fermanian J., Ginies P., Grun-Overdyking A., et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4) Pain. 2005;114:29–36. doi: 10.1016/j.pain.2004.12.010. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
