

Does the Heart Fall Asleep?-Diurnal Variations in Heart Rate Variability in Patients with Disorders of Consciousness
- PMID: 35326331
- PMCID: PMC8946070
- DOI: 10.3390/brainsci12030375
Does the Heart Fall Asleep?-Diurnal Variations in Heart Rate Variability in Patients with Disorders of Consciousness
Abstract
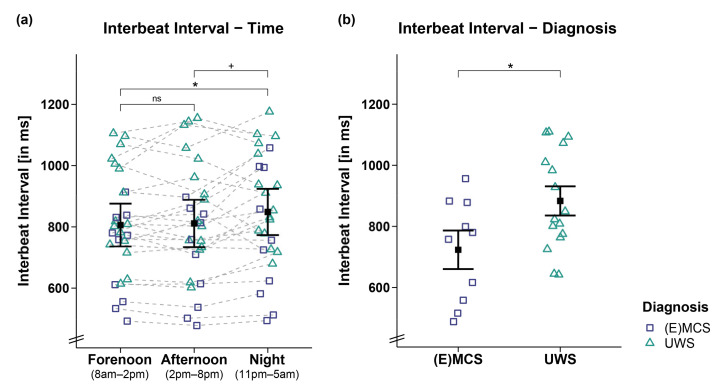
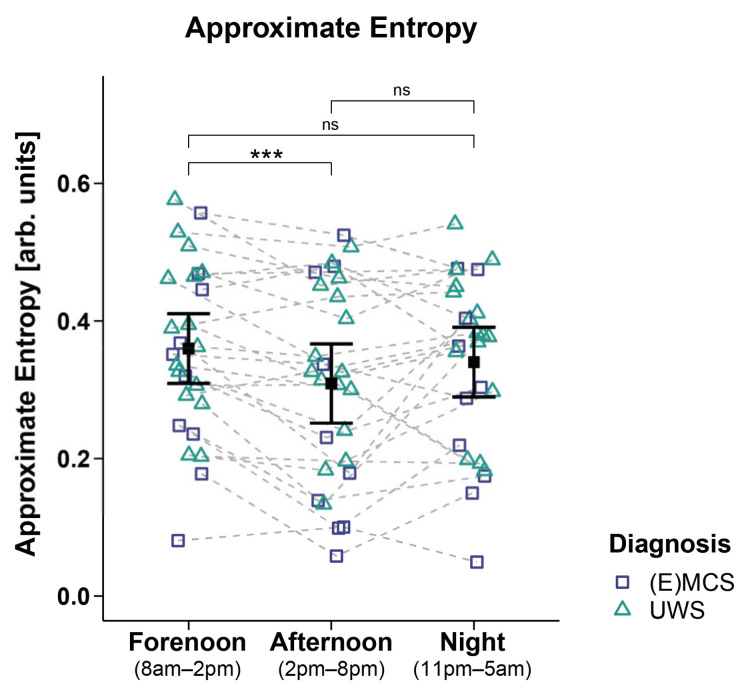
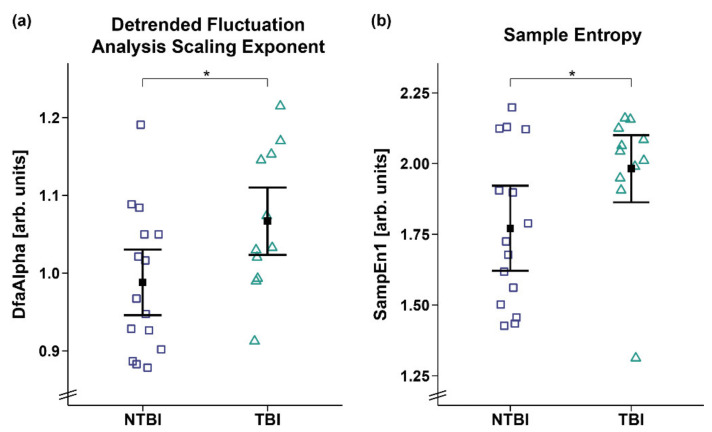
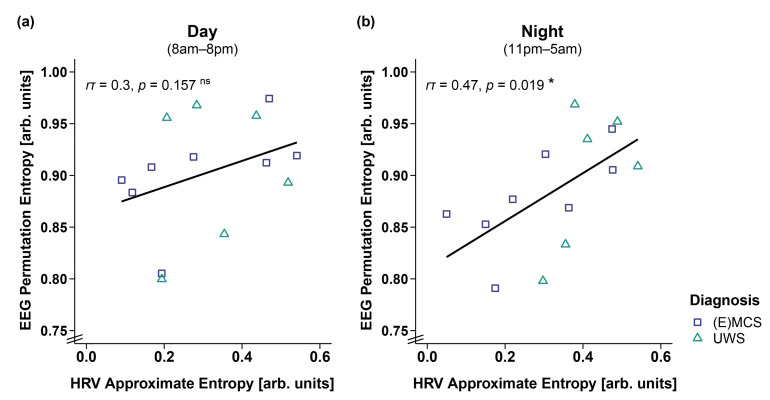
The current study investigated heart rate (HR) and heart rate variability (HRV) across day and night in patients with disorders of consciousness (DOC). We recorded 24-h electrocardiography in 26 patients with DOC (i.e., unresponsive wakefulness syndrome (UWS; n = 16) and (exit) minimally conscious state ((E)MCS; n = 10)). To examine diurnal variations, HR and HRV indices in the time, frequency, and entropy domains were computed for periods of clear day- (forenoon: 8 a.m.-2 p.m.; afternoon: 2 p.m.-8 p.m.) and nighttime (11 p.m.-5 a.m.). The results indicate that patients' interbeat intervals (IBIs) were larger during the night than during the day, indicating HR slowing. The patients in UWS showed larger IBIs compared to the patients in (E)MCS, and the patients with non-traumatic brain injury showed lower HRV entropy than the patients with traumatic brain injury. Additionally, higher HRV entropy was associated with higher EEG entropy during the night. Thus, cardiac activity varies with a diurnal pattern in patients with DOC and can differentiate between patients' diagnoses and etiologies. Moreover, the interaction of heart and brain appears to follow a diurnal rhythm. Thus, HR and HRV seem to mirror the integrity of brain functioning and, consequently, might serve as supplementary measures for improving the validity of assessments in patients with DOC.
Keywords: ECG; brain injury; disorders of consciousness; diurnal variation; heart rate; heart rate variability.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Laureys S., Celesia G.G., Cohadon F., Lavrijsen J., Leon-Carrion J., Sannita W.G., Sazbon L., Schmutzhard E., von Wild K.R., Zeman A., et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010;8:1–4. doi: 10.1186/1741-7015-8-68. - DOI - PMC - PubMed
-
- Bruno M.A., Vanhaudenhuyse A., Thibaut A., Moonen G., Laureys S. From unresponsive wakefulness to minimally conscious PLUS and functional locked-in syndromes: Recent advances in our understanding of disorders of consciousness. J. Neurol. 2011;258:1373–1384. doi: 10.1007/s00415-011-6114-x. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
