

BTK Inhibitors Impair Platelet-Mediated Antifungal Activity
- PMID: 35326454
- PMCID: PMC8947638
- DOI: 10.3390/cells11061003
BTK Inhibitors Impair Platelet-Mediated Antifungal Activity
Abstract
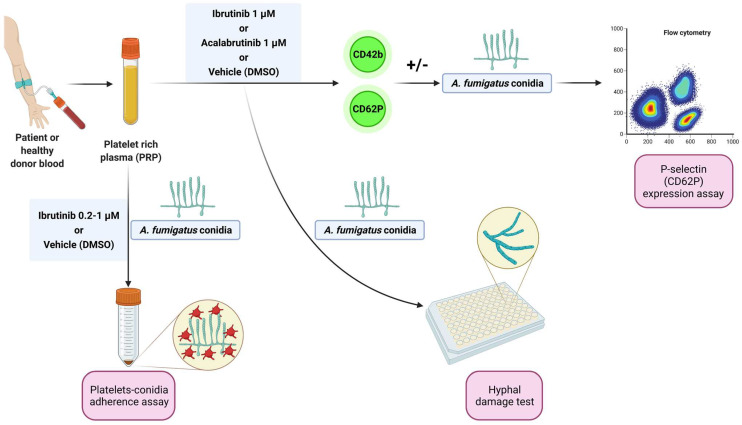
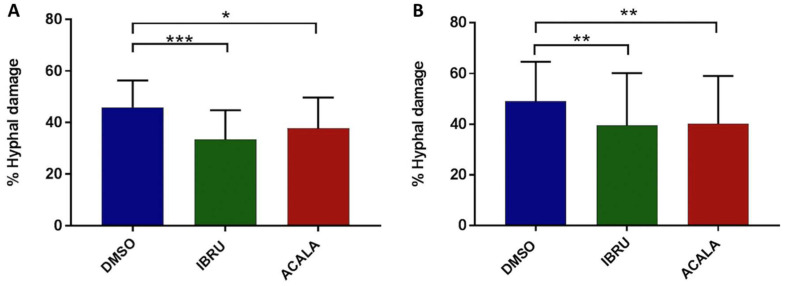
In recent years, the introduction of new drugs targeting Bruton's tyrosine kinase (BTK) has allowed dramatic improvement in the prognosis of patients with chronic lymphocytic leukemia (CLL) and other B-cell neoplasms. Although these small molecules were initially considered less immunosuppressive than chemoimmunotherapy, an increasing number of reports have described the occurrence of unexpected opportunistic fungal infections, in particular invasive aspergillosis (IA). BTK represents a crucial molecule in several signaling pathways depending on different immune receptors. Based on a variety of specific off-target effects on innate immunity, namely on neutrophils, monocytes, pulmonary macrophages, and nurse-like cells, ibrutinib has been proposed as a new host factor for the definition of probable invasive pulmonary mold disease. The role of platelets in the control of fungal growth, through granule-dependent mechanisms, was described in vitro almost two decades ago and is, so far, neglected by experts in the field of clinical management of IA. In the present study, we confirm the antifungal role of platelets, and we show, for the first time, that the exposure to BTK inhibitors impairs several immune functions of platelets in response to Aspergillus fumigatus, i.e., the ability to adhere to conidia, activation (as indicated by reduced expression of P-selectin), and direct killing activity. In conclusion, our experimental data suggest that antiplatelet effects of BTK inhibitors may contribute to an increased risk for IA in CLL patients.
Keywords: Aspergillus; BTK inhibitors; CLL; acalabrutinib; ibrutinib; invasive fungal infections; molds; platelets.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures




References
-
- Williams A.M., Baran A.M., Meacham P.J., Feldman M.M., Valencia H.E., Newsom-Stewart C., Gupta N., Janelsins M.C., Barr P.M., Zent C.S. Analysis of the Risk of Infection in Patients with Chronic Lymphocytic Leukemia in the Era of Novel Therapies. Leuk. Lymphoma. 2018;59:625–632. doi: 10.1080/10428194.2017.1347931. - DOI - PubMed
-
- Visentin A., Nasillo V., Marchetti M., Ferrarini I., Paolini R., Sancetta R., Rigolin G.M., Cibien F., Riva M., Briani C., et al. Clinical Characteristics and Outcome of West Nile Virus Infection in Patients with Lymphoid Neoplasms: An Italian Multicentre Study. Hemasphere. 2020;4:e395. doi: 10.1097/HS9.0000000000000395. - DOI - PMC - PubMed
-
- Ball S., Das A., Vutthikraivit W., Edwards P.J., Hardwicke F., Short N.J., Borthakur G., Maiti A. Risk of Infection Associated With Ibrutinib in Patients With B-Cell Malignancies: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Lymphoma Myeloma Leuk. 2020;20:87–97.e5. doi: 10.1016/j.clml.2019.10.004. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
