

Circulating Tumor DNA Profiling of a Diffuse Large B Cell Lymphoma Patient with Secondary Acute Myeloid Leukemia
- PMID: 35326522
- PMCID: PMC8946858
- DOI: 10.3390/cancers14061371
Circulating Tumor DNA Profiling of a Diffuse Large B Cell Lymphoma Patient with Secondary Acute Myeloid Leukemia
Abstract
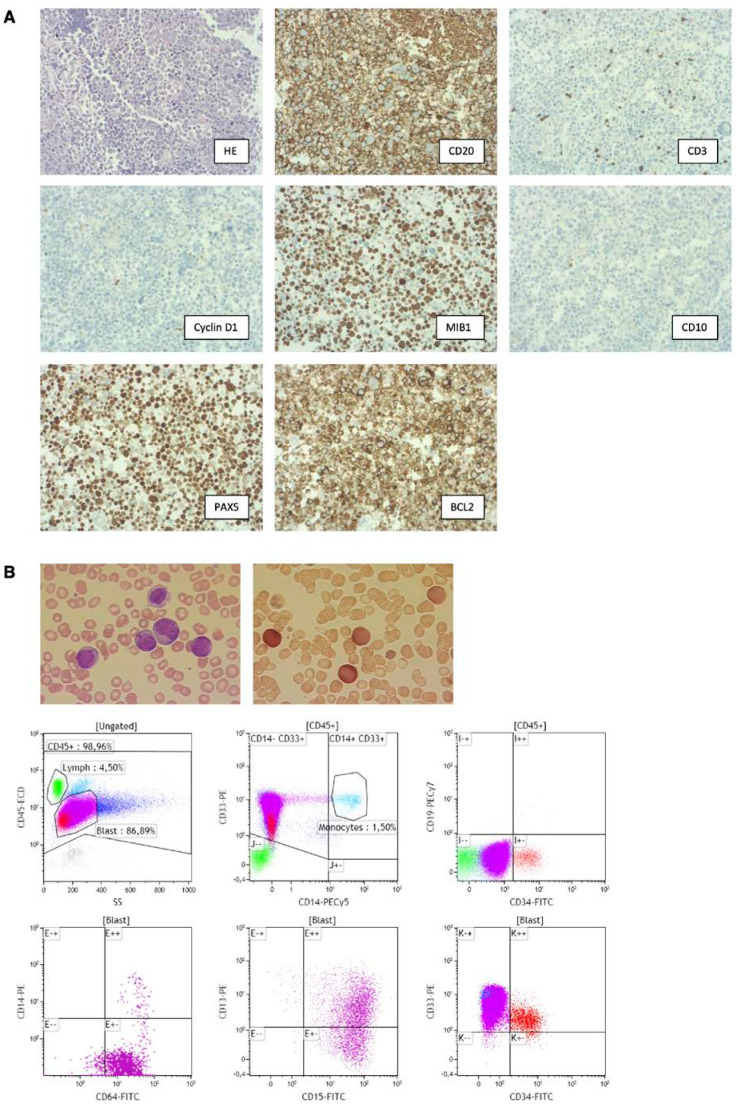
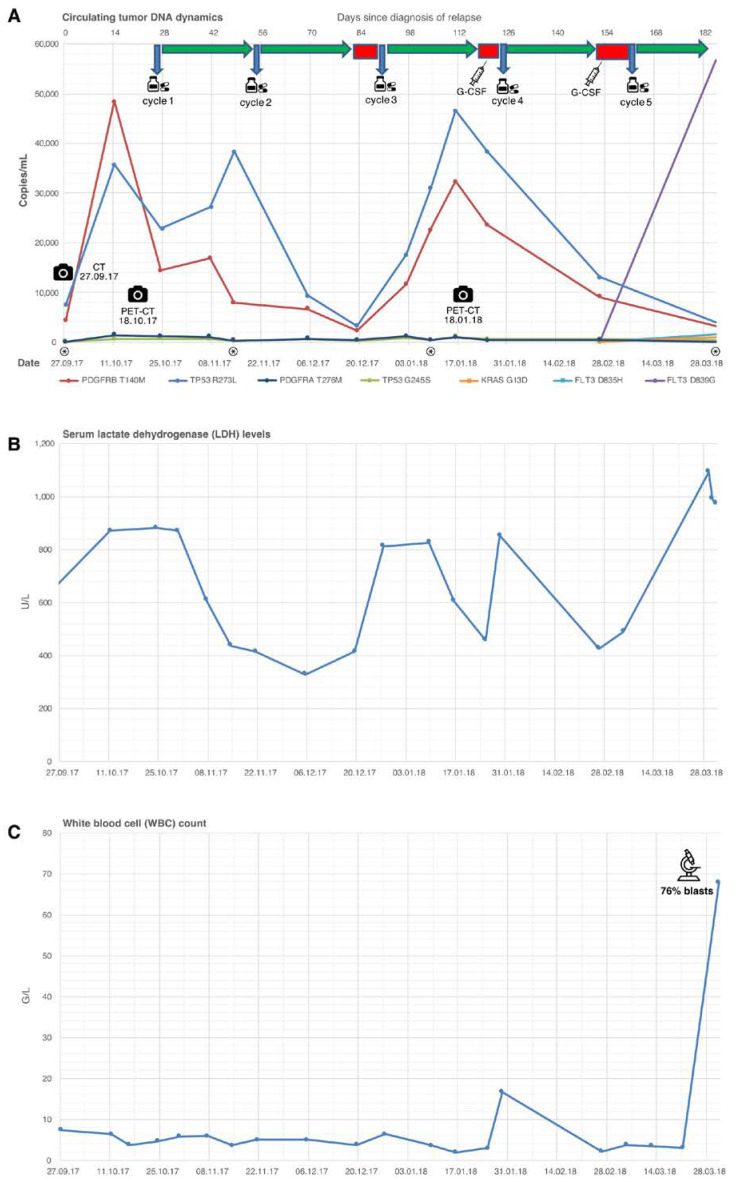
Diffuse large B cell lymphomas (DLBCL) are the most common neoplasia of the lymphatic system. Circulating cell-free DNA released from tumor cells (ctDNA) has been studied in many tumor entities and successfully used to monitor treatment and follow up. Studies of ctDNA in DLBCL so far have mainly focused on tracking mutations in peripheral blood initially detected by next-generation sequencing (NGS) of tumor tissue from one lymphoma manifestation site. This approach, however, cannot capture the mutational heterogeneity of different tumor sites in its entirety. In this case report, we present repetitive targeted next-generation sequencing combined with digital PCR out of peripheral blood of a patient with DLBCL relapse. By combining both detection methods, we were able to detect a new dominant clone of ctDNA correlating with the development of secondary therapy-related acute myeloid leukemia (t-AML) during the course of observation. Conclusively, our case report reinforces the diagnostic importance of ctDNA in DLBCL as well as the importance of repeated ctDNA sequencing combined with focused digital PCR assays to display the dynamic mutational landscape during the clinical course.
Keywords: cell-free DNA; digital PCR; liquid biopsy; precision medicine.
Conflict of interest statement
N.P. received advisory board and speaker fees from BMS, Novartis, Lilly, Bayer, AstraZeneca, Roche, Illumina, Thermo Fisher Scientific. F.B. has no competing financial interests. All other authors have no conflict of interests to declare.
Figures

Similar articles
-
Serial surveillance by circulating tumor DNA profiling after chimeric antigen receptor T therapy for the guidance of r/r diffuse large B cell lymphoma precise treatment.J Cancer. 2021 Jul 13;12(18):5423-5431. doi: 10.7150/jca.60390. eCollection 2021. J Cancer. 2021. PMID: 34405005 Free PMC article.
-
Genotyping on ctDNA Identifies Shifts in Mutation Spectrum Between Newly Diagnosed and Relapse/Refractory DLBCL.Onco Targets Ther. 2020 Oct 23;13:10797-10806. doi: 10.2147/OTT.S275334. eCollection 2020. Onco Targets Ther. 2020. PMID: 33122918 Free PMC article.
-
Liquid biopsy in hematological malignancies: current and future applications.Front Oncol. 2023 Apr 20;13:1164517. doi: 10.3389/fonc.2023.1164517. eCollection 2023. Front Oncol. 2023. PMID: 37152045 Free PMC article. Review.
-
Targeted Next-Generation Sequencing of Circulating Tumor DNA, Bone Marrow, and Peripheral Blood Mononuclear Cells in Pediatric AML.Front Oncol. 2021 Jul 29;11:666470. doi: 10.3389/fonc.2021.666470. eCollection 2021. Front Oncol. 2021. PMID: 34422630 Free PMC article.
-
Circulating Tumor DNA to Monitor Therapy for Aggressive B-Cell Lymphomas.Curr Treat Options Oncol. 2016 Sep;17(9):47. doi: 10.1007/s11864-016-0425-1. Curr Treat Options Oncol. 2016. PMID: 27461036 Review.
Cited by
-
Advancing Leukemia Management Through Liquid Biopsy: Insights into Biomarkers and Clinical Utility.Cancers (Basel). 2025 Apr 25;17(9):1438. doi: 10.3390/cancers17091438. Cancers (Basel). 2025. PMID: 40361366 Free PMC article. Review.
References
-
- Sant M., Allemani C., Tereanu C., De Angelis R., Capocaccia R., Visser O., Marcos-Gragera R., Maynadié M., Simonetti A., Lutz J.M., et al. Incidence of hematologic malignancies in Europe by morphologic subtype: Results of the HAEMACARE project. Blood. 2010;116:3724–3734. doi: 10.1182/blood-2010-05-282632. - DOI - PubMed
-
- Barrington S.F., Mikhaeel N.G., Kostakoglu L., Meignan M., Hutchings M., Müeller S.P., Schwartz L.H., Zucca E., Fisher R.I., Trotman J., et al. Role of Imaging in the Staging and Response Assessment of Lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014;32:3048–3058. doi: 10.1200/JCO.2013.53.5229. - DOI - PMC - PubMed
-
- Tilly H., da Silva M.G., Vitolo U., Jack A., Meignan M., Lopez-Guillermo A., Walewski J., André M., Johnson P.W., Pfreundschuh M., et al. Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015;26((Suppl. 5)):v116–v125. doi: 10.1093/annonc/mdv304. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
