

Similar Outcomes in Minimally Invasive versus Open Management of Primary Pancreatic Neuroendocrine Tumors: A Regional, Multi-Institutional Collaborative Analysis
- PMID: 35326539
- PMCID: PMC8946133
- DOI: 10.3390/cancers14061387
Similar Outcomes in Minimally Invasive versus Open Management of Primary Pancreatic Neuroendocrine Tumors: A Regional, Multi-Institutional Collaborative Analysis
Abstract
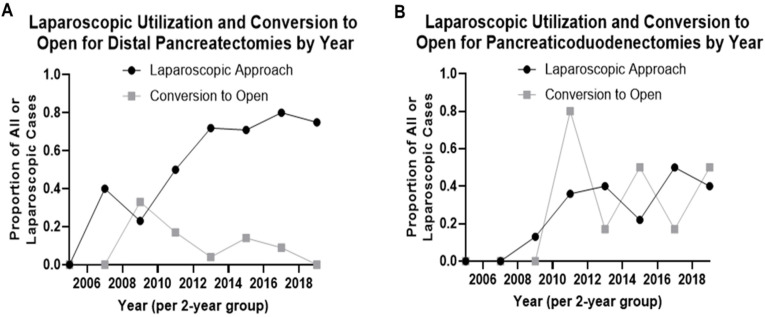
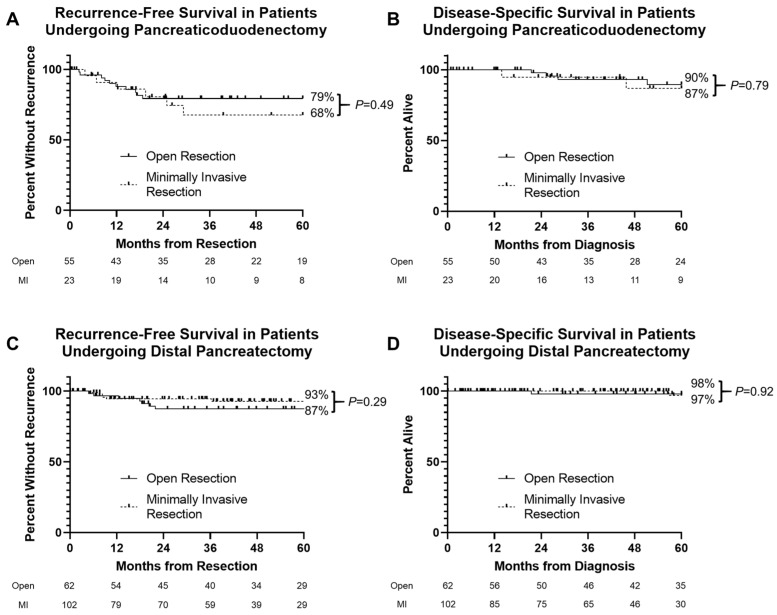
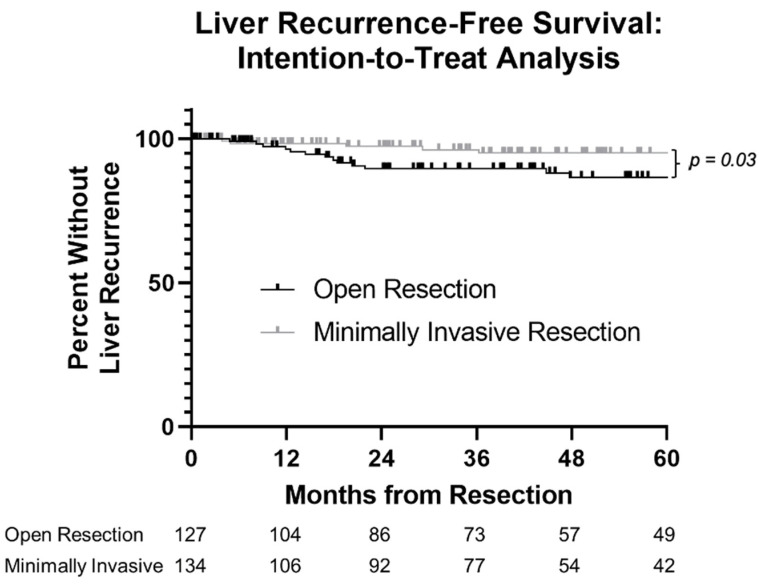
In pancreatic neuroendocrine tumors (PNETs), the impact of minimally invasive (MI) versus open resection on outcomes remains poorly studied. We queried a multi-institutional pancreatic cancer registry for patients with resected non-metastatic PNET from 1996−2020. Recurrence-free (RFS), disease-specific survival (DSS), and operative complications were evaluated. Two hundred and eighty-two patients were identified. Operations were open in 139 (49%) and MI in 143 (51%). Pancreaticoduodenectomy was performed in 77 (27%, n = 23 MI), distal pancreatectomy in 184 (65%, n = 109 MI), enucleation in 13 (5%), and total pancreatectomy in eight (3%). Median follow-up was 50 months. Thirty-six recurrences and 13 deaths from recurrent disease yielded 5-year RFS and DSS of 85% and 95%, respectively. On multivariable analysis, grade 1 (HR 0.07, p < 0.001) and grade 2 (HR 0.20, p = 0.002) tumors were associated with improved RFS, while T3/T4 tumors were associated with worse RFS (OR 2.78, p = 0.04). MI resection was not associated with RFS (HR 0.53, p = 0.14). There was insufficient mortality to evaluate DSS with multivariable analysis. Of 159 patients with available NSQIP data, incisional surgical site infections (SSIs), organ space SSIs, Grade B/C pancreatic fistulas, reoperations, and need for percutaneous drainage did not differ by operative approach (all p > 0.2). Nodal harvest was similar for MI versus open distal pancreatectomies (p = 0.16) and pancreaticoduodenectomies (p = 0.28). Minimally invasive surgical management of PNETs is equivalent for oncologic and postoperative outcomes.
Keywords: minimally invasive surgery; oncologic outcomes; pancreatic neuroendocrine tumor; perioperative outcomes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Pancreatic Neuroendocrine Tumors: What Is the Best Surgical Option?J Clin Med. 2024 May 20;13(10):3015. doi: 10.3390/jcm13103015. J Clin Med. 2024. PMID: 38792555 Free PMC article. Review.
-
Minimally Invasive vs Open Pancreatectomy for Pancreatic Neuroendocrine Tumors: Multi-Institutional 10-Year Experience of 1,023 Patients.J Am Coll Surg. 2022 Aug 1;235(2):315-330. doi: 10.1097/XCS.0000000000000257. Epub 2022 May 2. J Am Coll Surg. 2022. PMID: 35839409
-
Minimally Invasive Versus Open Pancreatectomy for Right-Sided and Left-Sided G1/G2 Nonfunctioning Pancreatic Neuroendocrine Tumors: A Multicenter Matched Analysis with an Inverse Probability of Treatment-Weighting Method.Ann Surg Oncol. 2021 Nov;28(12):7742-7758. doi: 10.1245/s10434-021-10092-0. Epub 2021 May 9. Ann Surg Oncol. 2021. PMID: 33969463
-
Minimally invasive vs open pancreatectomy for nonfunctioning pancreatic neuroendocrine tumors.World J Gastrointest Oncol. 2020 Oct 15;12(10):1133-1145. doi: 10.4251/wjgo.v12.i10.1133. World J Gastrointest Oncol. 2020. PMID: 33133382 Free PMC article.
-
Pre- and intraoperative diagnostic requirements, benefits and risks of minimally invasive and robotic surgery for neuroendocrine tumors of the pancreas.Best Pract Res Clin Endocrinol Metab. 2019 Oct;33(5):101294. doi: 10.1016/j.beem.2019.101294. Epub 2019 Jul 10. Best Pract Res Clin Endocrinol Metab. 2019. PMID: 31351817 Review.
Cited by
-
Robotic Versus Laparoscopic Versus Open Surgery for Non-Metastatic Pancreatic Neuroendocrine Tumors (pNETs): A Systematic Review and Network Meta-Analysis.J Clin Med. 2024 Oct 22;13(21):6303. doi: 10.3390/jcm13216303. J Clin Med. 2024. PMID: 39518444 Free PMC article. Review.
-
Pancreatic Neuroendocrine Tumors: What Is the Best Surgical Option?J Clin Med. 2024 May 20;13(10):3015. doi: 10.3390/jcm13103015. J Clin Med. 2024. PMID: 38792555 Free PMC article. Review.
-
Contemporary Approaches to the Surgical Management of Pancreatic Neuroendocrine Tumors.Cancers (Basel). 2024 Apr 14;16(8):1501. doi: 10.3390/cancers16081501. Cancers (Basel). 2024. PMID: 38672582 Free PMC article. Review.
References
-
- Cuschieri A. Laparoscopic Surgery of the Pancreas. J. R. Coll. Surg. Edinb. 1994;39:178–184. - PubMed
LinkOut - more resources
Full Text Sources
