

Periprosthetic Joint Infection (PJI)-Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone-A Retrospective Cohort Study
- PMID: 35326773
- PMCID: PMC8944641
- DOI: 10.3390/antibiotics11030310
Periprosthetic Joint Infection (PJI)-Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone-A Retrospective Cohort Study
Abstract
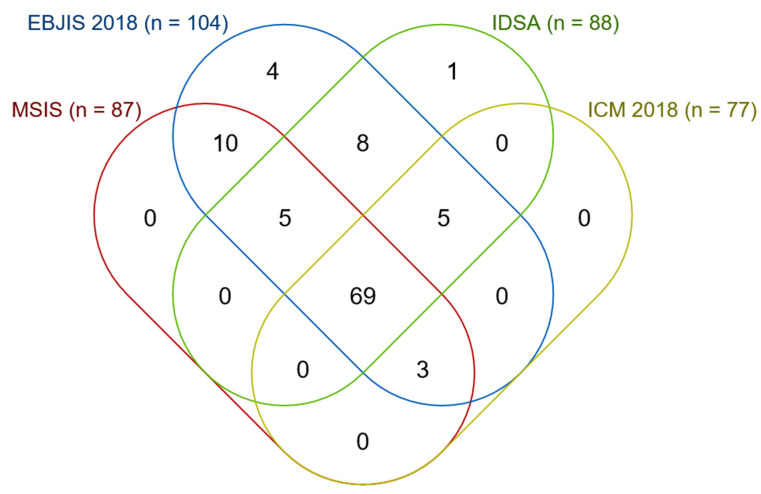
Controversy exists regarding the optimal treatment of periprosthetic joint infection (PJI), considering control of infection, functional results as well as quality of life. Difficulties in treatment derive from the formation of biofilms within a few days after infection. Biofilms are tolerant to systemically applied antibiotics, requiring extreme concentrations for a prolonged period. Minimum biofilm eradicating concentrations (MBEC) are only feasible by the local application of antibiotics. One established approach is the use of allograft bone as a carrier, granting a sustained release of antibiotics in very high concentrations after appropriate impregnation. The purpose of this study was to determine the rate of reinfection after a one-stage revision of infected hip or knee prostheses, using antibiotic-impregnated allograft bone as the carrier and avoiding cement. Between 1 January 2004 and 31 January 2018, 87 patients with PJI, according to MSIS, underwent a one-stage revision with antibiotic-impregnated cancellous allograft bone. An amount of 17 patients had insufficient follow-ups. There were 70 remaining patients (34 male, 36 female) with a mean follow-up of 5.6 years (range 2-15.6) and with a mean age of 68.2 years (range 31.5-86.9). An amount of 38 hips and 11 knees were implanted without any cement; and 21 knees were implanted with moderate cementing at the articular surface with stems always being uncemented. Within 2 years after surgery, 6 out of 70 patients (8.6%, CI 2-15.1) showed reinfection and after more than 2 years, an additional 6 patients showed late-onset infection. Within 2 years after surgery, 11 out of 70 patients (15.7%, CI 7.2-24.2) had an implant failure for any reason (including infection) and after more than 2 years, an additional 7 patients had an implant failure. Using Kaplan-Meier analysis for all 87 patients, the estimated survival for reinfection was 93.9% (CI 88.8-99.1) at 1 year, 89.9% (CI 83.2-96.6) at 2 years and 81.5% (CI 72.1-90.9) at 5 years. The estimated survival for implant failure for any reason was 90.4% (CI 84.1-96.7) at 1 year, 80.9% (CI 72.2-89.7) at 2 years and 71.1% (CI 60.3-81.8) at 5 years. One-stage revision with antibiotic-impregnated cancellous allograft bone grants comparable results regarding infection control as with multiple stages, while shortening rehabilitation, improving quality of life for the patients and reducing costs for the health care system.
Keywords: antibiotic carrier; antibiotic-impregnated cancellous allograft bone; biofilm; cementless implants; impaction grafting; local antimicrobial therapy; microorganism; one-stage revision; periprosthetic joint infection; single-stage.
Conflict of interest statement
H.W. is a consultant for LIMA spa and the director of AllogenRx. H.W was a former president of ECTB. G.D. declares no conflict of interest.
Figures



Similar articles
-
Rationale for one stage exchange of infected hip replacement using uncemented implants and antibiotic impregnated bone graft.Int J Med Sci. 2009 Sep 4;6(5):247-52. doi: 10.7150/ijms.6.247. Int J Med Sci. 2009. PMID: 19834590 Free PMC article. Review.
-
[ANTIBIOTIC-IMPREGNATED ARTICULAR CEMENT SPACER FOR TREATMENT OF PERIPROSTHETIC JOINT INFECTION].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015 Apr;29(4):420-5. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015. PMID: 26477151 Chinese.
-
Irrigation, Débridement, and Implant Retention for Recurrence of Periprosthetic Joint Infection Following Two-Stage Revision Total Knee Arthroplasty: A Matched Cohort Study.J Arthroplasty. 2019 Aug;34(8):1772-1775. doi: 10.1016/j.arth.2019.04.009. Epub 2019 Apr 10. J Arthroplasty. 2019. PMID: 31060919
-
Bone grafting and one-stage revision of THR - biological reconstruction and effective antimicrobial treatment using antibiotic impregnated allograft bone.Hip Int. 2012 Jul-Aug;22 Suppl 8:S62-8. doi: 10.5301/HIP.2012.9572. Hip Int. 2012. PMID: 22956385
-
Outcome of Revision Surgery for Infection After Total Knee Arthroplasty: Results of 3 Surgical Strategies.JBJS Rev. 2019 Jun;7(6):e4. doi: 10.2106/JBJS.RVW.18.00084. JBJS Rev. 2019. PMID: 31188156 Review.
Cited by
-
Efficacy and safety of intra-articular-only meropenem after one-stage revision for treating Escherichia coli-induced periprosthetic joint infection in a rat model.Bone Joint Res. 2024 Oct 4;13(10):546-558. doi: 10.1302/2046-3758.1310.BJR-2024-0119.R1. Bone Joint Res. 2024. PMID: 39362652 Free PMC article.
References
LinkOut - more resources
Full Text Sources
