

An 18-Year Dataset on the Clinical Incidence and MICs to Antibiotics of Achromobacter spp. (Labeled Biochemically or by MAL-DI-TOF MS as A. xylosoxidans), Largely in Patient Groups Other than Those with CF
- PMID: 35326774
- PMCID: PMC8944543
- DOI: 10.3390/antibiotics11030311
An 18-Year Dataset on the Clinical Incidence and MICs to Antibiotics of Achromobacter spp. (Labeled Biochemically or by MAL-DI-TOF MS as A. xylosoxidans), Largely in Patient Groups Other than Those with CF
Abstract
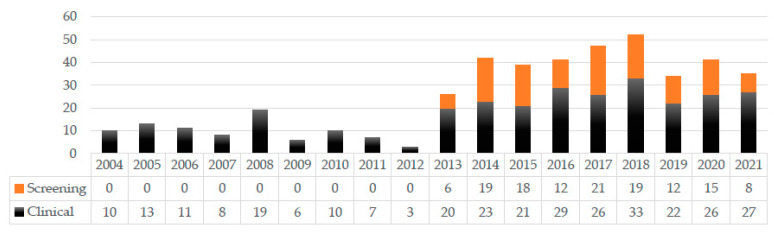
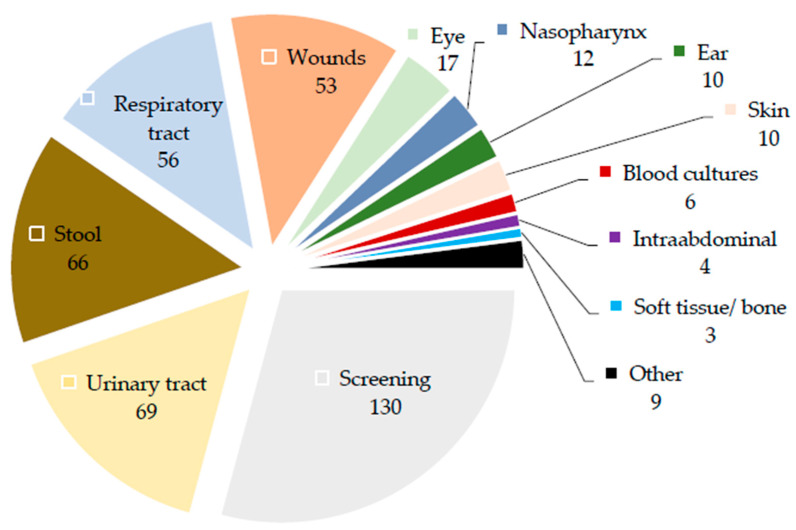
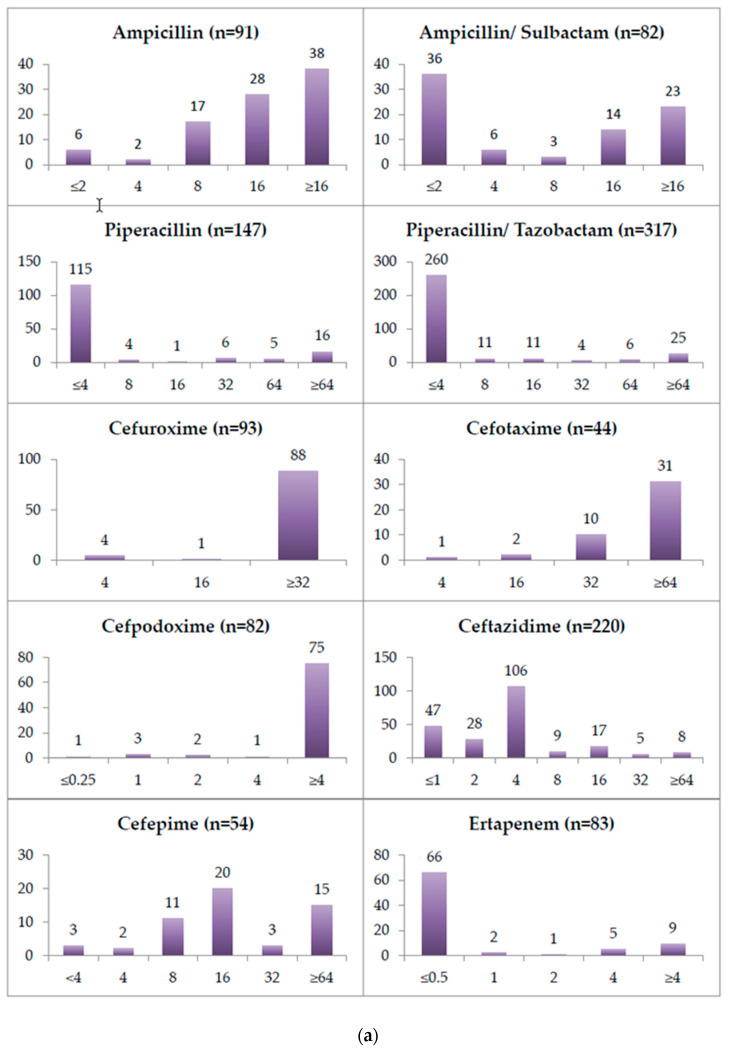
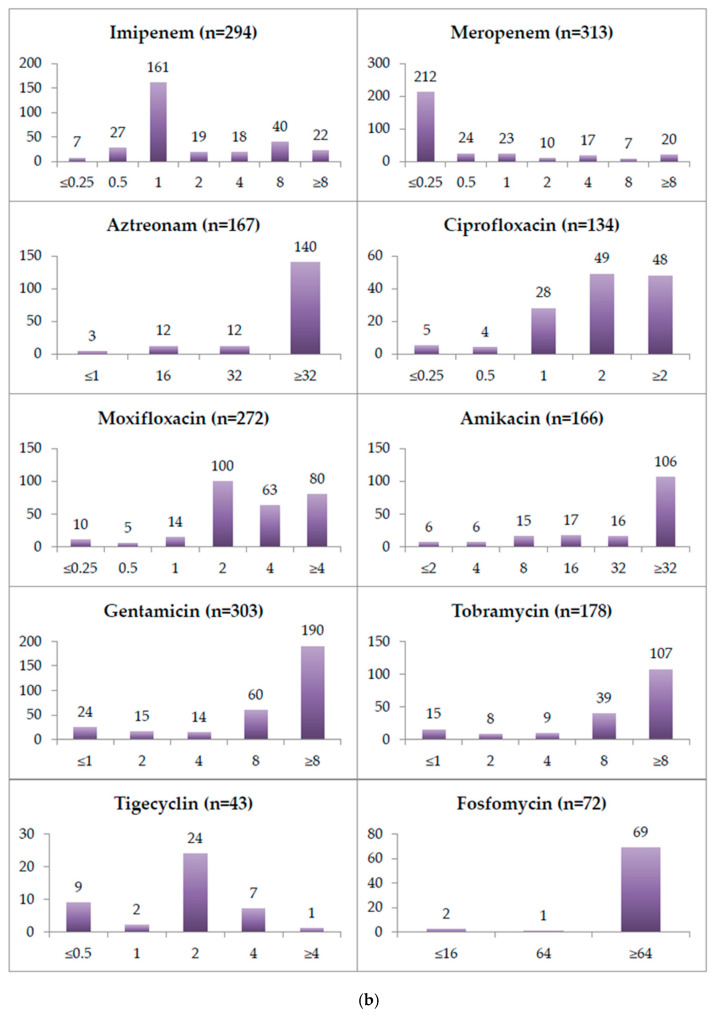
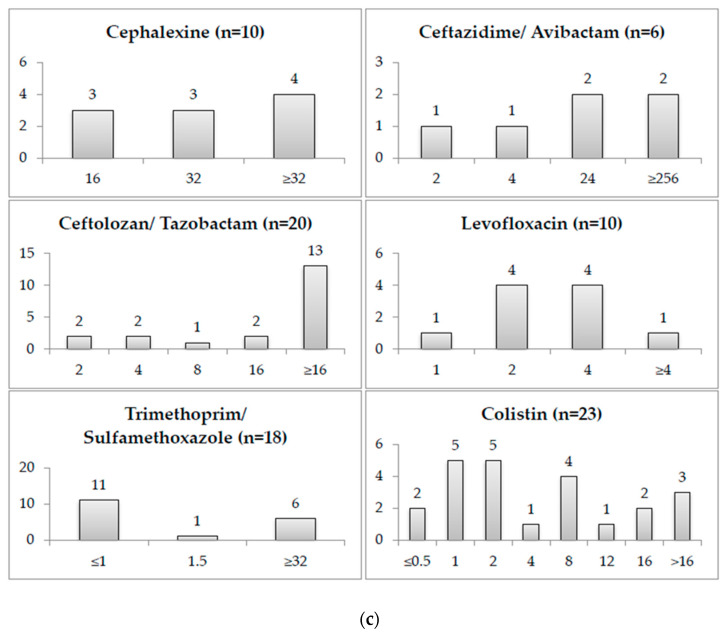
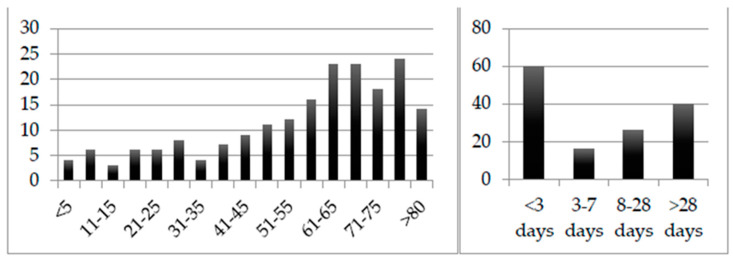
Achromobacter spp. are intrinsically multidrug-resistant environmental microorganisms which are known to cause opportunistic, nosocomial, and sometimes chronic infections. The existing literature yields scarcely any larger datasets, especially with regard to the incidence in patient groups other than those with cystic fibrosis. The aim of this study was to fill this gap. We present a retrospective analysis of 314 clinical and 130 screening isolates detected in our diagnostic unit between 2004 and 2021, combined with patients' demographic and clinical information (ward type and length of hospitalization), and the results of routine diagnostic antibiotic MIC determination. We found the apparent increase in prevalence in our diagnostic unit, in which cystic fibrosis patients are an underrepresented group, in large part to be attributable to an overall increase in the number of samples and, more importantly, changes in the diagnostic setting, such as the introduction of rigorous screening for Gram-negative multidrug-resistant pathogens. We found these Achromobacter spp. to be most commonly detected in urine, stool, wounds and airway samples, and found the resistance rates to vary strongly between different sample types. Intestinal carriage is frequently not investigated, and its frequency is likely underestimated. Isolates resistant to meropenem can hardly be treated.
Keywords: Achromobacter; Achromobacter xylosoxidans; Alcaligenaceae; Burkholderiales; antibiotic resistance; emerging pathogens; non-fermenting Gram-negative bacilli; nosocomial pathogens; opportunistic pathogens.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Chronic Airway Colonization by Achromobacter xylosoxidans in Cystic Fibrosis Patients Is Not Sustained by Their Domestic Environment.Appl Environ Microbiol. 2018 Nov 15;84(23):e01739-18. doi: 10.1128/AEM.01739-18. Print 2018 Dec 1. Appl Environ Microbiol. 2018. PMID: 30217850 Free PMC article.
-
Achromobacter xylosoxidans is the predominant Achromobacter species isolated from diverse non-respiratory samples.Epidemiol Infect. 2016 Dec;144(16):3527-3530. doi: 10.1017/S0950268816001564. Epub 2016 Aug 18. Epidemiol Infect. 2016. PMID: 27535588 Free PMC article.
-
Pan-Resistant Achromobacter xylosoxidans and Stenotrophomonas maltophilia Infection in Cystic Fibrosis Does Not Reduce Survival After Lung Transplantation.Transplantation. 2015 Oct;99(10):2196-202. doi: 10.1097/TP.0000000000000709. Transplantation. 2015. PMID: 25856407
-
Epidemic Achromobacter xylosoxidans strain among Belgian cystic fibrosis patients and review of literature.BMC Microbiol. 2016 Jun 24;16(1):122. doi: 10.1186/s12866-016-0736-1. BMC Microbiol. 2016. PMID: 27342812 Free PMC article. Review.
-
Antibiotic treatment of multidrug-resistant organisms in cystic fibrosis.Am J Respir Med. 2003;2(4):321-32. doi: 10.1007/BF03256660. Am J Respir Med. 2003. PMID: 14719998 Review.
Cited by
-
Development of a Simple and Accurate Molecular Protocol Using 16SrRNA for Species-Specific Identification of Achromobacter spp.Pathogens. 2025 Mar 12;14(3):271. doi: 10.3390/pathogens14030271. Pathogens. 2025. PMID: 40137756 Free PMC article.
-
ESKAPEE Pathogen Biofilm Control on Surfaces with Probiotic Lactobacillaceae and Bacillus species.Antibiotics (Basel). 2023 May 8;12(5):871. doi: 10.3390/antibiotics12050871. Antibiotics (Basel). 2023. PMID: 37237774 Free PMC article. Review.
-
Identification of Virulence Factors Involved in a Murine Model of Severe Achromobacter xylosoxidans Infection.Infect Immun. 2023 Jul 18;91(7):e0003723. doi: 10.1128/iai.00037-23. Epub 2023 May 31. Infect Immun. 2023. PMID: 37255468 Free PMC article.
-
The In Vitro Replication Cycle of Achromobacter xylosoxidans and Identification of Virulence Genes Associated with Cytotoxicity in Macrophages.Microbiol Spectr. 2022 Aug 31;10(4):e0208322. doi: 10.1128/spectrum.02083-22. Epub 2022 Jul 20. Microbiol Spectr. 2022. PMID: 35856670 Free PMC article.
-
Comparative phenotypic and genotypic antimicrobial susceptibility surveillance in Achromobacter spp. through whole genome sequencing.Microbiol Spectr. 2025 Apr;13(4):e0252724. doi: 10.1128/spectrum.02527-24. Epub 2025 Feb 27. Microbiol Spectr. 2025. PMID: 40013782 Free PMC article.
References
-
- Pressler T., Høiby N., Gormsen M. Chronic infection with Achromobacter xylosoxidans in cystic fibrosis patients; a retrospective case control study. J. Cyst. Fibros. 2006;5:245–251. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
