

Short and Concise Peer-to-Peer Teaching-Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion
- PMID: 35326866
- PMCID: PMC8944614
- DOI: 10.3390/antibiotics11030402
Short and Concise Peer-to-Peer Teaching-Example of a Successful Antibiotic Stewardship Intervention to Increase Iv to Po Conversion
Abstract
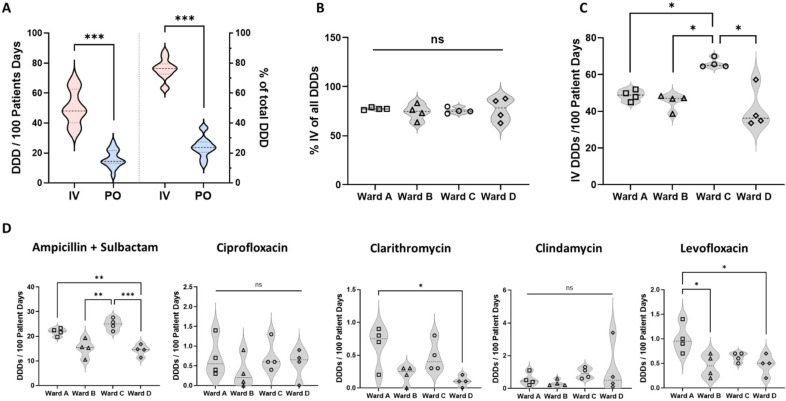
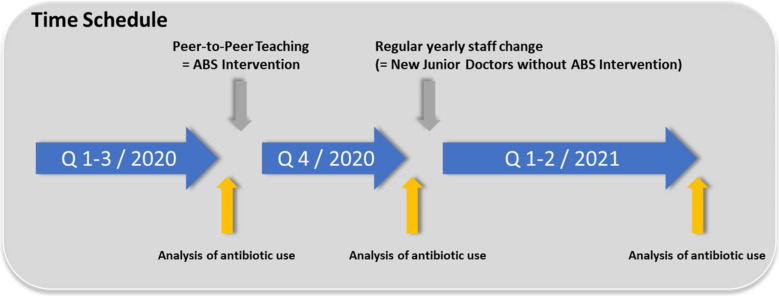
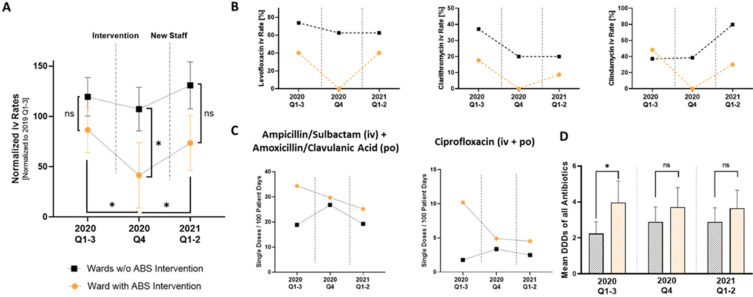
Antibiotic stewardship (ABS) programs aim to combine effective treatment with minimized antibiotic-related harms. Common ABS interventions are simple and effective, but their implementation in daily practice is often difficult. The aim of our study was to investigate if a single, short, peer-to-peer teaching intervention (junior doctor to junior doctor) during clinical routine can successfully improve antibiotic prescriptions. We performed a quasi-experimental before-after study on a regular care cardiology ward at a large academic medical center in Germany. We evaluated antibiotic use metrics retrospectively and calculated defined daily doses (DDD) with the anatomical therapeutic chemical/DDD classification system of the World Health Organization. We hypothesize that the over-representative use of intravenous administration is a potentially modifiable target, which can be proven by antibiotic use metrics analysis. After a single peer-to-peer teaching session with a focus on indications for iv to po conversion, the normalized percentage of intravenous compared to oral administration significantly decreased (from 86.5 ± 50.3% to 41.4 ± 70.3%). Moreover, after the intervention, antibiotics with high oral bioavailability were no longer administered intravenously at all during the following quarter. Our results indicate that even a single peer-to-peer training session is highly effective in improving the iv to po conversion rate in the short term.
Keywords: antibiotic prescribing; antibiotic stewardship; antibiotic use; defined daily doses; peer-to-peer teaching.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Implementation of a Clinical Decision Support Tool to Improve Antibiotic IV-to-Oral Conversion Rates at a Community Academic Hospital.Can J Hosp Pharm. 2019 Nov-Dec;72(6):455-461. Epub 2019 Dec 1. Can J Hosp Pharm. 2019. PMID: 31853146 Free PMC article.
-
Impact and barriers of a pharmacist-led practice with computerized reminders on intravenous to oral antibiotic conversion for community-acquired pneumonia inpatients.J Clin Pharm Ther. 2021 Aug;46(4):1055-1061. doi: 10.1111/jcpt.13397. Epub 2021 Jun 7. J Clin Pharm Ther. 2021. PMID: 34101230
-
The use of an IV to PO clinical intervention form to improve antibiotic administration in a community based hospital.BMJ Qual Improv Rep. 2015 Jan 28;4(1):u200786.w2247. doi: 10.1136/bmjquality.u200786.w2247. eCollection 2015. BMJ Qual Improv Rep. 2015. PMID: 26734367 Free PMC article.
-
Addressing Concerns about Changing the Route of Antimicrobial Administration from Intravenous to Oral in Adult Inpatients.Can J Hosp Pharm. 2015 Jul-Aug;68(4):318-26. doi: 10.4212/cjhp.v68i4.1472. Can J Hosp Pharm. 2015. PMID: 26327706 Free PMC article. Review.
-
[Antibiotic stewardship (ABS)-strategies for urologists in private practice and hospitals].Urologe A. 2020 Dec;59(12):1472-1479. doi: 10.1007/s00120-020-01385-5. Urologe A. 2020. PMID: 33201296 Free PMC article. Review. German.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
