

Two-Month Individually Supervised Exercise Therapy Improves Walking Speed, Step Length, and Temporal Gait Symmetry in Chronic Stroke Patients: A before-after Trial
- PMID: 35327005
- PMCID: PMC8951068
- DOI: 10.3390/healthcare10030527
Two-Month Individually Supervised Exercise Therapy Improves Walking Speed, Step Length, and Temporal Gait Symmetry in Chronic Stroke Patients: A before-after Trial
Abstract
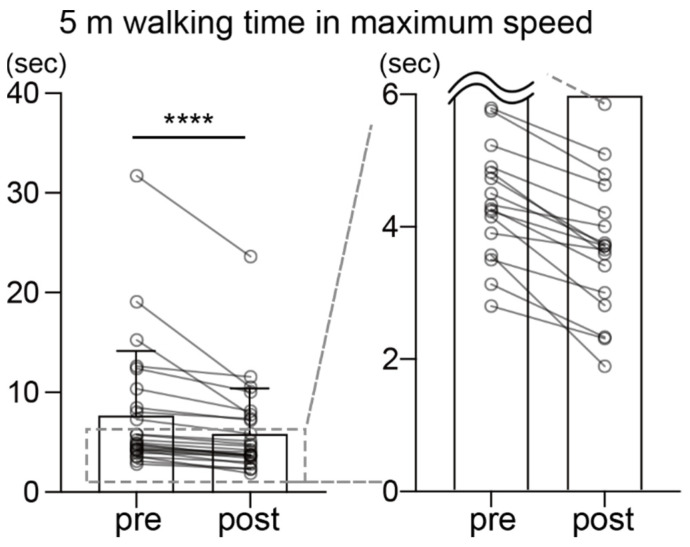
Gait asymmetry is common after stroke and is a major risk factor for falls. In particular, temporal gait asymmetry often remains in the chronic stage of stroke. However, health insurance does not cover rehabilitation for patients with chronic stroke in many countries. Accordingly, it is undetermined whether individually supervised exercise therapy has beneficial effects on chronic hemiparetic gait. Patients with stroke (n = 25) more than 6 months after onset performed 70 min of individually supervised exercise twice weekly for 2 months in 16 sessions with qualified personnel. The intervention significantly reduced the pre-swing phase on the paretic side (mean = 91.8%, 95%CI, 84.8−98.8). In addition, there was a significant improvement in pre-swing phase symmetry in those with great asymmetry prior to the intervention (p = 0.022). Step length significantly increased after the intervention on both sides (non-paretic, p = 0.029; paretic, p = 0.0055). Walking time at both comfortable and maximum speeds was significantly shortened (comfortable, p = 0.0041; maximum, p < 0.0001). Our findings suggest that there remains scope to improve gait ability with individually supervised exercise therapy in patients with chronic stroke, whose functional recovery is often considered unlikely. This type of intervention may be a simple and effective option to improve gait parameters, including temporal asymmetry, even in patients with chronic stroke.
Keywords: chronic phase; exercise therapy; gait asymmetry; hemiparesis; stroke.
Conflict of interest statement
M.Y., K.I., K.H. (Kimikazu Honda) and K.H. (Koshiro Hayashida) are employees of SENSTYLE Inc.
Figures



Similar articles
-
Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds.Gait Posture. 2005 Aug;22(1):51-6. doi: 10.1016/j.gaitpost.2004.06.009. Gait Posture. 2005. PMID: 15996592
-
Gait recovery is not associated with changes in the temporal patterning of muscle activity during treadmill walking in patients with post-stroke hemiparesis.Clin Neurophysiol. 2006 Jan;117(1):4-15. doi: 10.1016/j.clinph.2005.08.014. Epub 2005 Dec 5. Clin Neurophysiol. 2006. PMID: 16337186 Clinical Trial.
-
Gait asymmetry pattern following stroke determines acute response to locomotor task.Gait Posture. 2020 Mar;77:300-307. doi: 10.1016/j.gaitpost.2020.02.016. Epub 2020 Feb 26. Gait Posture. 2020. PMID: 32126493 Free PMC article.
-
Paretic propulsion as a measure of walking performance and functional motor recovery post-stroke: A review.Gait Posture. 2019 Feb;68:6-14. doi: 10.1016/j.gaitpost.2018.10.027. Epub 2018 Oct 25. Gait Posture. 2019. PMID: 30408710 Free PMC article. Review.
-
High Intensity Exercise for Walking Competency in Individuals with Stroke: A Systematic Review and Meta-Analysis.J Stroke Cerebrovasc Dis. 2019 Dec;28(12):104414. doi: 10.1016/j.jstrokecerebrovasdis.2019.104414. Epub 2019 Sep 27. J Stroke Cerebrovasc Dis. 2019. PMID: 31570262
Cited by
-
Effect of Anterioposterior Weight-Shift Training with Visual Biofeedback in Patients with Step Length Asymmetry after Subacute Stroke.J Pers Med. 2023 Dec 18;13(12):1726. doi: 10.3390/jpm13121726. J Pers Med. 2023. PMID: 38138953 Free PMC article.
References
-
- Feigin V.L., Nichols E., Alam T., Bannick M.S., Beghi E., Blake N., Culpepper W.J., RayDorsey E., Elbaz A., Ellenbogen R.G., et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18:459–480. doi: 10.1016/S1474-4422(18)30499-X. - DOI - PMC - PubMed
-
- SLord E., McPherson K., McNaughton H.K., Rochester L., Weatherall M. Community ambulation after stroke: How important and obtainable is it and what measures appear predictive? Arch. Phys. Med. Rehabil. 2004;85:234–239. - PubMed
-
- Han E.Y., Im S.H., Kim B.R., Seo M.J., Kim M.O. Robot-assisted gait training improves brachial-ankle pulse wave velocity and peak aerobic capacity in subacute stroke patients with totally dependent ambulation: Randomized controlled trial. Medicine. 2016;95:e5078. doi: 10.1097/MD.0000000000005078. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
