

ICG-Guided Lymphadenectomy during Surgery for Colon and Rectal Cancer-Interim Analysis of the GREENLIGHT Trial
- PMID: 35327344
- PMCID: PMC8945555
- DOI: 10.3390/biomedicines10030541
ICG-Guided Lymphadenectomy during Surgery for Colon and Rectal Cancer-Interim Analysis of the GREENLIGHT Trial
Abstract
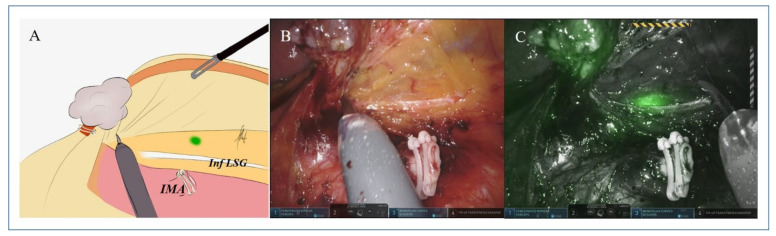
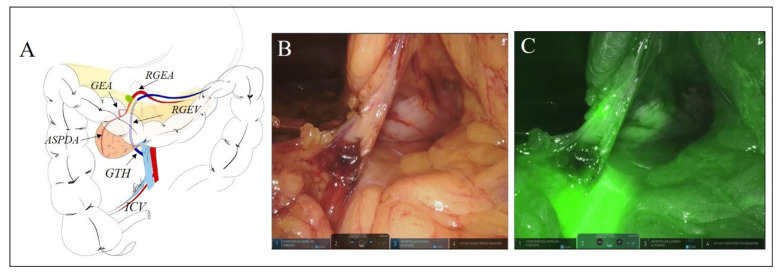
Lymphadenectomy is crucial for an optimal oncologic resection of colon and rectal cancers. However, without a direct visualization, an aberrant route of lymph node (LN) diffusion might remain unresected. Indocyanine-green (ICG) lymphatic mapping permits a real-time LNs visualization. We designed the GREENLIGHT trial to explore in 100 patients undergoing robotic colorectal resection the clinical significance of a D3 ICG-guided lymphadenectomy. The primary endpoint was the number of patients in whom ICG changed the extent of lymphadenectomy. We report herein the interim analysis on the first 70 patients. After endoscopic ICG injection 24 h (n = 49) or 72 h (n = 21) ahead, 19, 20, and 31 patients underwent right colectomy, left colectomy, and anterior rectal resection. The extent of lymphadenectomy changed in 35 (50%) patients, mostly (29 (41.4%)) for the identification of LNs (median two) outside the standard draining basin. Identification of such LNs was less frequent in rectal tumors that had undergone chemoradiotherapy (26.3%) (p > 0.05). A non-significant correlation between time-to-ICG injection and identification of aberrant LNs was observed (48.9% at 24 h vs. 23.8% at 72 h). The presence of LN metastases did not affect a proper fluorescent mapping. These data indicate that ICG lymphatic mapping provides relevant information in 50% of patients, thus increasing the accuracy of potentially curative resections.
Keywords: ICG; ICG-guided lymphadenectomy; colorectal cancer; lymphatic mapping; robotic surgery.
Conflict of interest statement
G.S. is proctor for Intuitive Surgical, Inc., Sunnyvale, CA, USA. All other authors declare no conflict of interest. The funder had no role in the design of the study, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Moynihan B.G. The surgical treatment of cancer of the sigmoid flexure and rectum with especial reference to the principles to be observed. Surg. Gynecol. Obstet. 1908;6:463–466.
-
- Le Voyer T.E., Sigurdson E.R., Hanlon A.L., Mayer R.J., Macdonald J.S., Catalano P.J., Haller D.G. Colon cancer survival is associated with increasing number of lymph nodes analyzed: A secondary survey of intergroup trial INT-0089. J. Clin. Oncol. 2003;21:2912–2919. doi: 10.1200/JCO.2003.05.062. - DOI - PubMed
LinkOut - more resources
Full Text Sources
