

Inherited Retinal Degeneration: PARP-Dependent Activation of Calpain Requires CNG Channel Activity
- PMID: 35327647
- PMCID: PMC8946186
- DOI: 10.3390/biom12030455
Inherited Retinal Degeneration: PARP-Dependent Activation of Calpain Requires CNG Channel Activity
Abstract
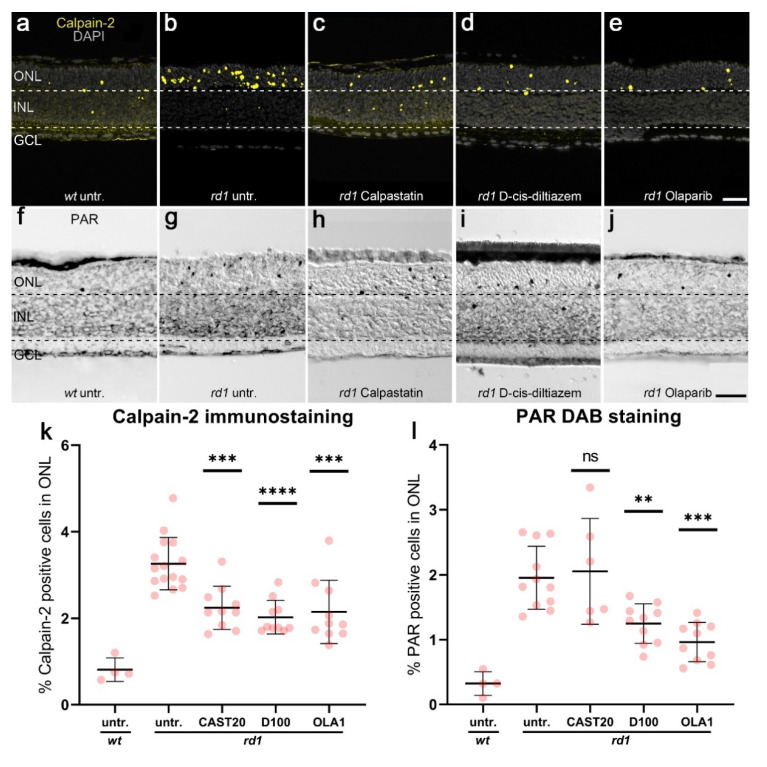
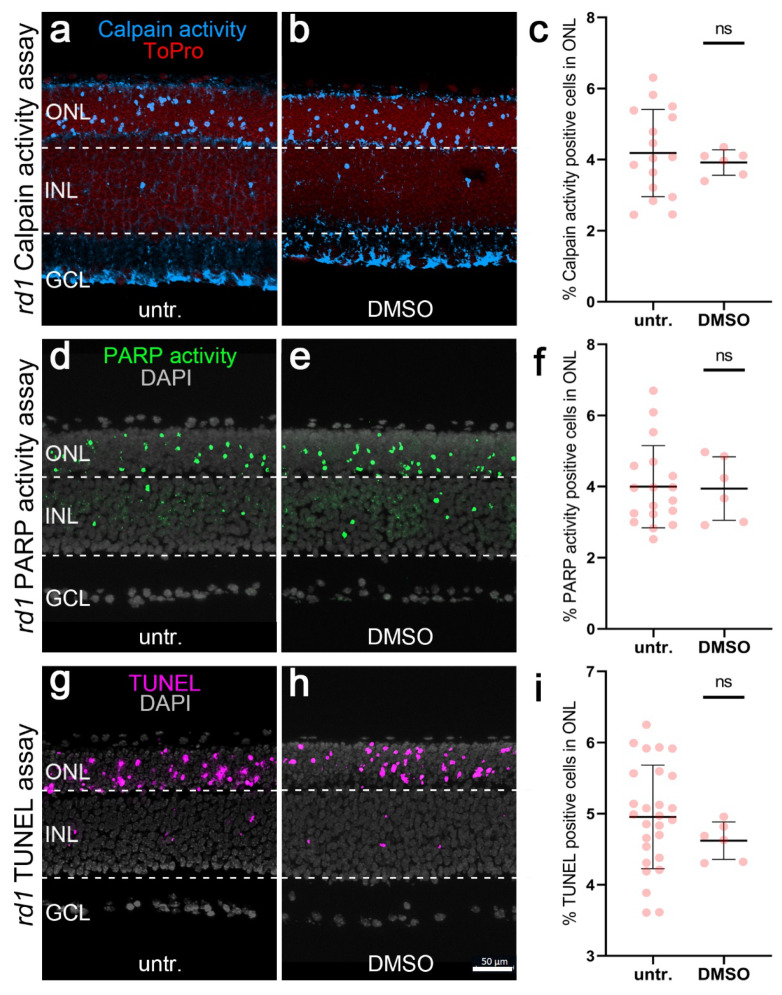
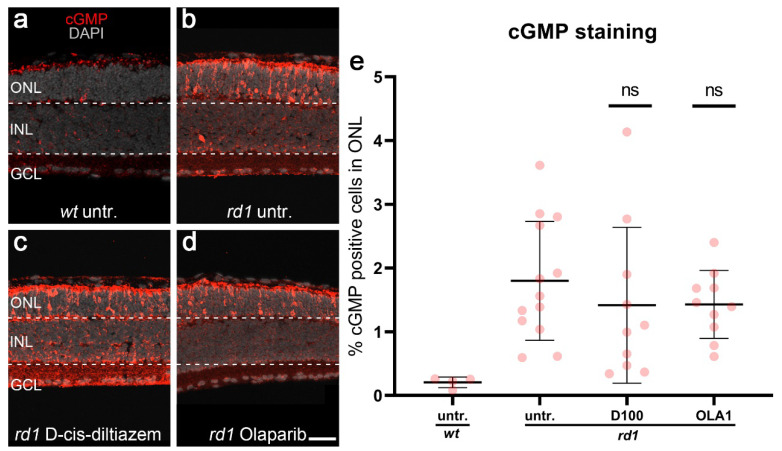
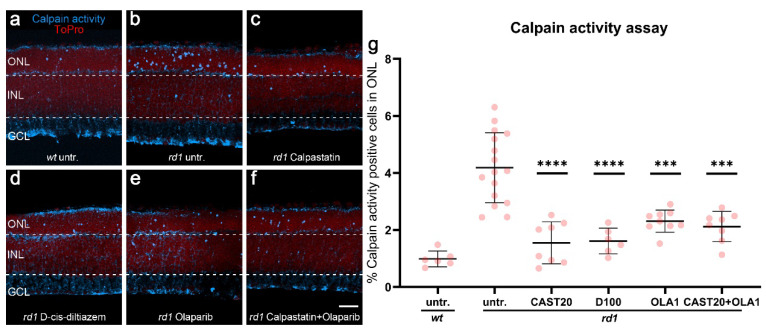
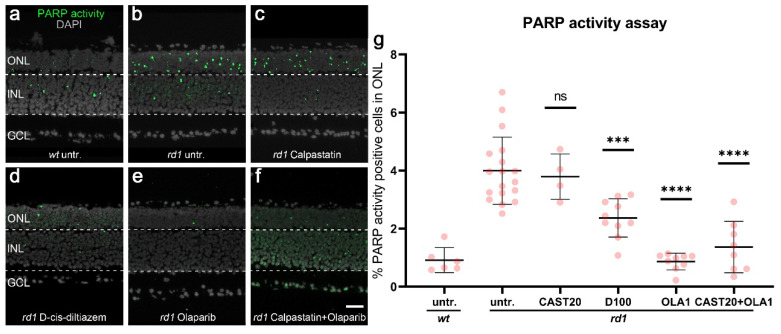
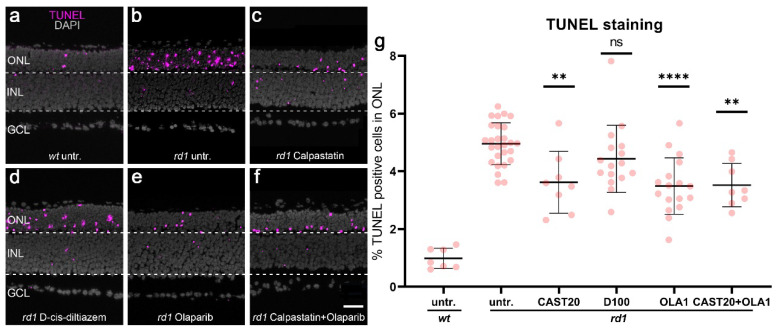
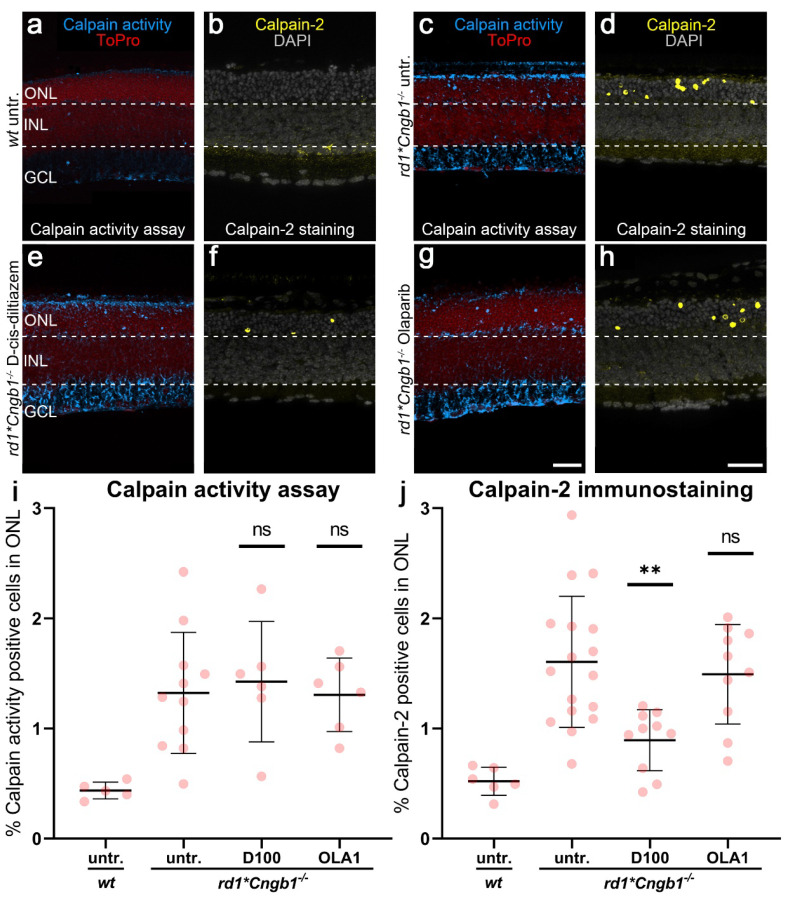
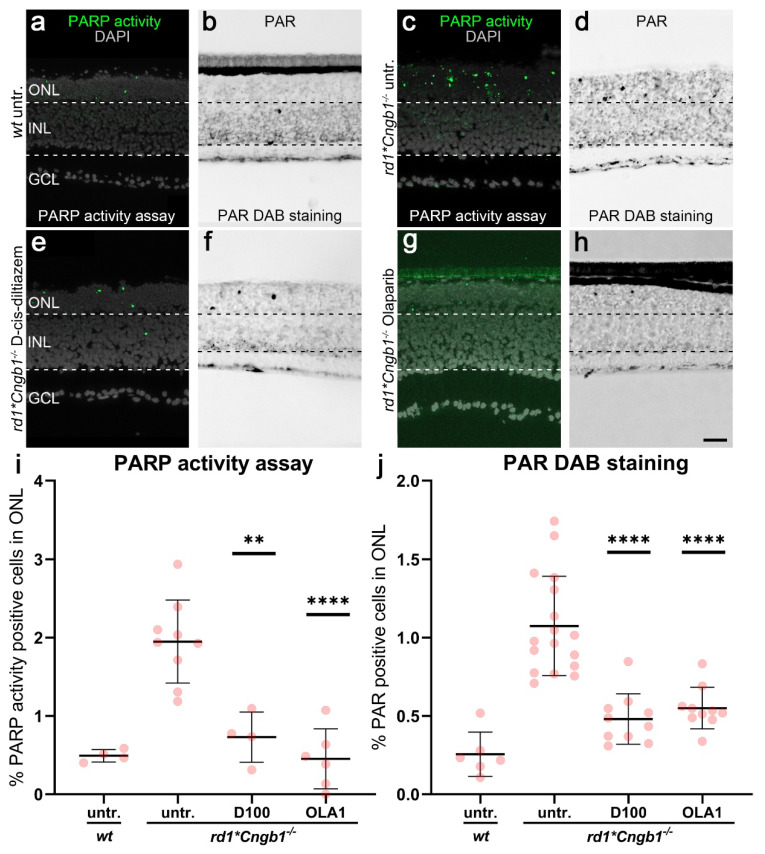
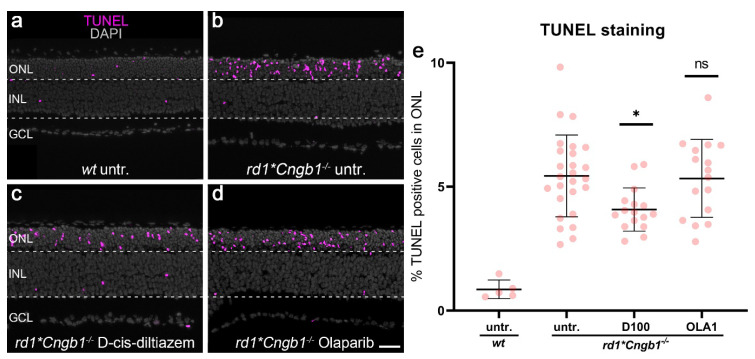
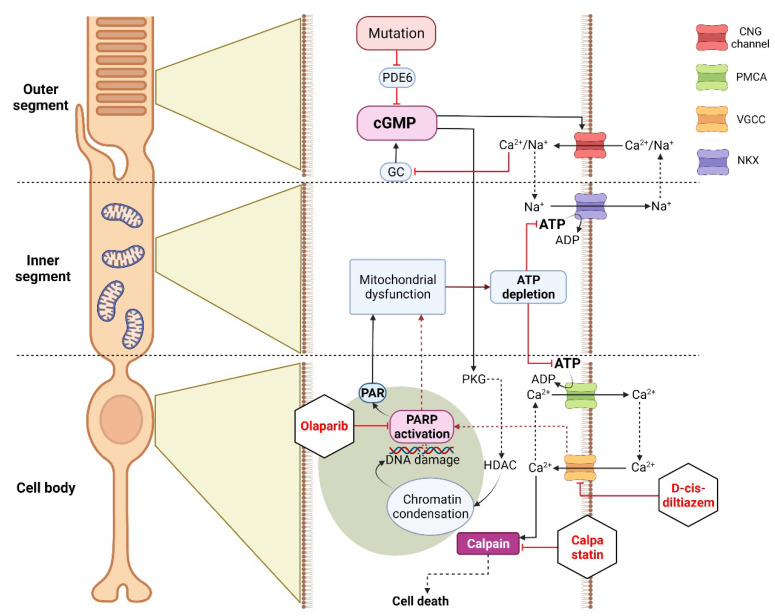
Inherited retinal degenerations (IRDs) are a group of blinding diseases, typically involving a progressive loss of photoreceptors. The IRD pathology is often based on an accumulation of cGMP in photoreceptors and associated with the excessive activation of calpain and poly (ADP-ribose) polymerase (PARP). Inhibitors of calpain or PARP have shown promise in preventing photoreceptor cell death, yet the relationship between these enzymes remains unclear. To explore this further, organotypic retinal explant cultures derived from wild-type and IRD-mutant mice were treated with inhibitors specific for calpain, PARP, and voltage-gated Ca2+ channels (VGCCs). The outcomes were assessed using in situ activity assays for calpain and PARP and immunostaining for activated calpain-2, poly (ADP-ribose), and cGMP, as well as the TUNEL assay for cell death detection. The IRD models included the Pde6b-mutant rd1 mouse and rd1*Cngb1-/- double-mutant mice, which lack the beta subunit of the rod cyclic nucleotide-gated (CNG) channel and are partially protected from rd1 degeneration. We confirmed that an inhibition of either calpain or PARP reduces photoreceptor cell death in rd1 retina. However, while the activity of calpain was decreased by the inhibition of PARP, calpain inhibition did not alter the PARP activity. A combination treatment with calpain and PARP inhibitors did not synergistically reduce cell death. In the slow degeneration of rd1*Cngb1-/- double mutant, VGCC inhibition delayed photoreceptor cell death, while PARP inhibition did not. Our results indicate that PARP acts upstream of calpain and that both are part of the same degenerative pathway in Pde6b-dependent photoreceptor degeneration. While PARP activation may be associated with CNG channel activity, calpain activation is linked to VGCC opening. Overall, our data highlights PARP as a target for therapeutic interventions in IRD-type diseases.
Keywords: HDAC; PKG; cGMP; calcium; nonapoptotic cell death; photoreceptor degeneration; retinitis pigmentosa.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Inherited Retinal Degeneration: Towards the Development of a Combination Therapy Targeting Histone Deacetylase, Poly (ADP-Ribose) Polymerase, and Calpain.Biomolecules. 2023 Mar 23;13(4):581. doi: 10.3390/biom13040581. Biomolecules. 2023. PMID: 37189329 Free PMC article.
-
T-type voltage-gated channels, Na+/Ca2+-exchanger, and calpain-2 promote photoreceptor cell death in inherited retinal degeneration.Cell Commun Signal. 2024 Feb 1;22(1):92. doi: 10.1186/s12964-023-01391-y. Cell Commun Signal. 2024. PMID: 38303059 Free PMC article.
-
Cav1.4 L-Type Calcium Channels Contribute to Calpain Activation in Degenerating Photoreceptors of rd1 Mice.PLoS One. 2016 Jun 7;11(6):e0156974. doi: 10.1371/journal.pone.0156974. eCollection 2016. PLoS One. 2016. PMID: 27270916 Free PMC article.
-
cGMP Signaling in Photoreceptor Degeneration.Int J Mol Sci. 2023 Jul 7;24(13):11200. doi: 10.3390/ijms241311200. Int J Mol Sci. 2023. PMID: 37446378 Free PMC article. Review.
-
Photoreceptor cell death mechanisms in inherited retinal degeneration.Mol Neurobiol. 2008 Dec;38(3):253-69. doi: 10.1007/s12035-008-8045-9. Epub 2008 Nov 4. Mol Neurobiol. 2008. PMID: 18982459 Review.
Cited by
-
Retinal Organoids from an AIPL1 CRISPR/Cas9 Knockout Cell Line Successfully Recapitulate the Molecular Features of LCA4 Disease.Int J Mol Sci. 2023 Mar 21;24(6):5912. doi: 10.3390/ijms24065912. Int J Mol Sci. 2023. PMID: 36982987 Free PMC article.
-
Single-Cell Transcriptomic Profiling in Inherited Retinal Degeneration Reveals Distinct Metabolic Pathways in Rod and Cone Photoreceptors.Int J Mol Sci. 2022 Oct 12;23(20):12170. doi: 10.3390/ijms232012170. Int J Mol Sci. 2022. PMID: 36293024 Free PMC article.
-
Zebrafish cdh23 Affects Rod Cell Phototransduction Through Regulating Ca2+ Transport and MAPK Signaling Pathway.Int J Mol Sci. 2025 May 11;26(10):4604. doi: 10.3390/ijms26104604. Int J Mol Sci. 2025. PMID: 40429749 Free PMC article.
-
Neuroprotection provided by polyphenols and flavonoids in photoreceptor degenerative diseases.Neural Regen Res. 2026 Mar 1;21(3):908-922. doi: 10.4103/NRR.NRR-D-24-01638. Epub 2025 May 6. Neural Regen Res. 2026. PMID: 40364630 Free PMC article.
-
Inherited Retinal Degeneration: Towards the Development of a Combination Therapy Targeting Histone Deacetylase, Poly (ADP-Ribose) Polymerase, and Calpain.Biomolecules. 2023 Mar 23;13(4):581. doi: 10.3390/biom13040581. Biomolecules. 2023. PMID: 37189329 Free PMC article.
References
-
- Duncan J.L., Pierce E.A., Laster A.M., Daiger S.P., Birch D.G., Ash J.D., Iannaccone A., Flannery J.G., Sahel J.A., Zack D.J., et al. Technology, Inherited retinal degenerations: Current landscape and knowledge gaps. Transl. Vis. Sci. Technol. 2018;74:6. doi: 10.1167/tvst.7.4.6. - DOI - PMC - PubMed
-
- Arango-Gonzalez B., Trifunović D., Sahaboglu A., Kranz K., Michalakis S., Farinelli P., Koch S., Koch F., Cottet S., Janssen-Bienhold U., et al. Identification of a common non-apoptotic cell death mechanism in hereditary retinal degeneration. PLoS ONE. 2014;9:e112142. doi: 10.1371/journal.pone.0112142. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
