

First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease-A Potential Novel Diagnostic Indicator
- PMID: 35328201
- PMCID: PMC8947148
- DOI: 10.3390/diagnostics12030648
First Characterization of ADAMTS-4 in Kidney Tissue and Plasma of Patients with Chronic Kidney Disease-A Potential Novel Diagnostic Indicator
Abstract
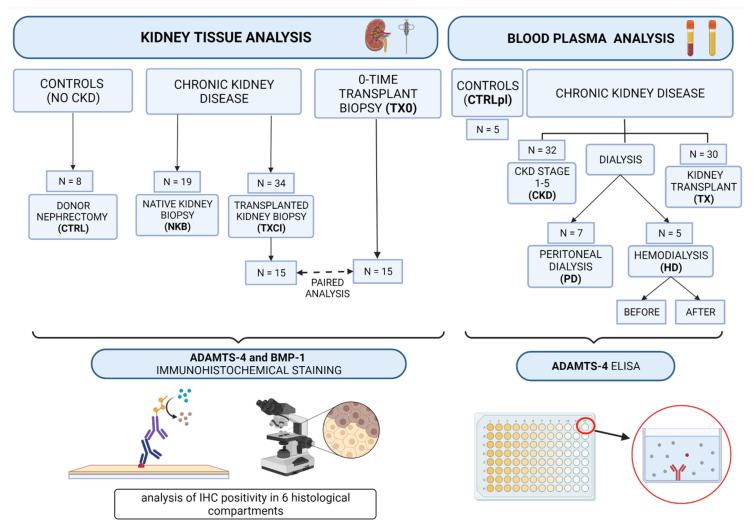
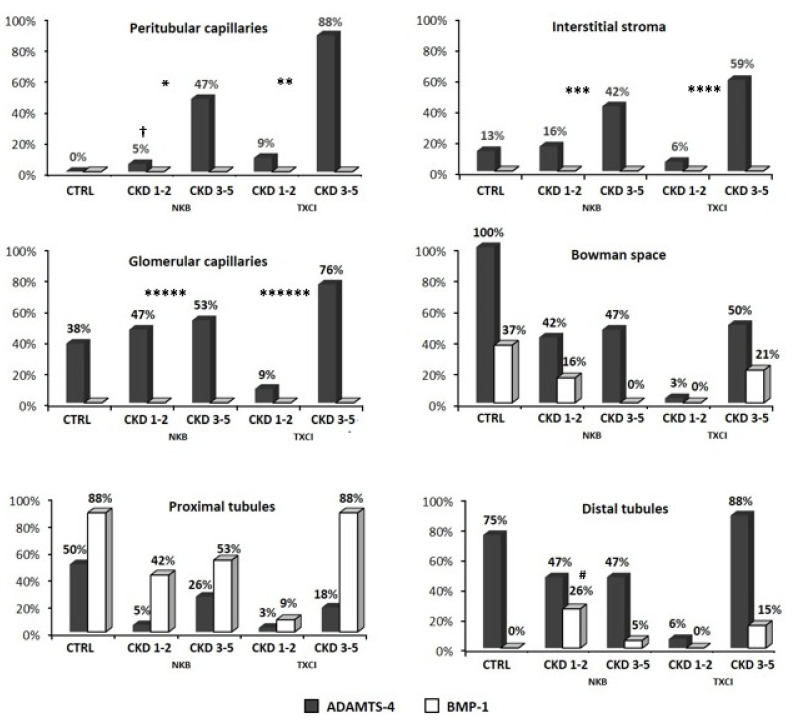
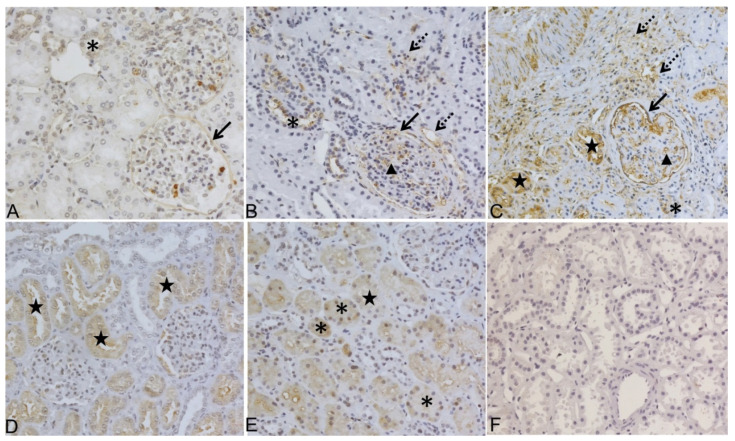
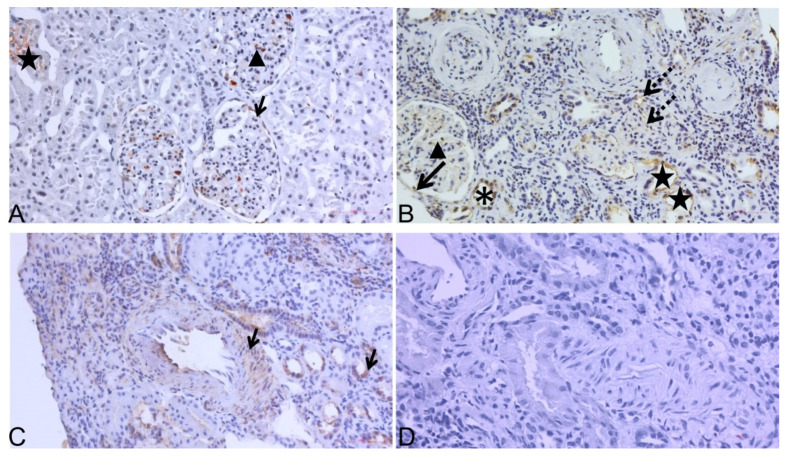
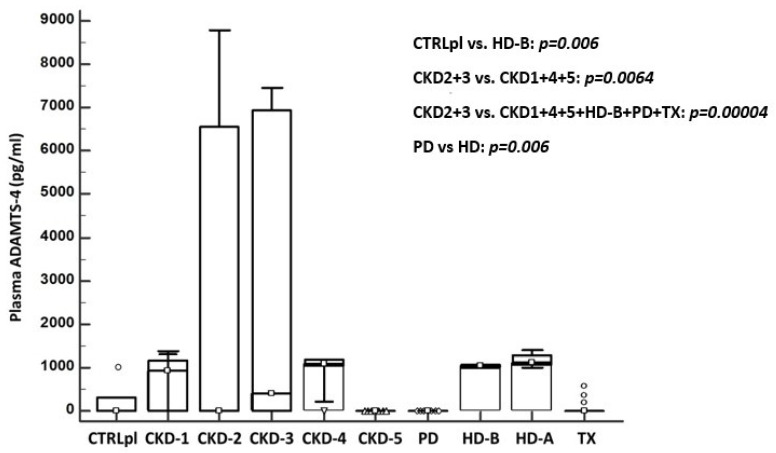
Background: We have previously shown that metzincin protease ADAMTS-4 accompanies renal fibrogenesis, as it appears in the blood of hemodialysis patients. Methods: Native kidney (NKB) and kidney transplant (TXCI) biopsy samples as well as plasma from patients with various stages of CKD were compared to controls. In paired analysis, 15 TXCI samples were compared with their zero-time biopsies (TX0). Tissues were evaluated and scored (interstitial fibrosis and tubular atrophy (IFTA) for NKB and Banff ci for TXCI). Immunohistochemical (IHC) staining for ADAMTS-4 and BMP-1 was performed. Plasma ADAMTS-4 was detected using ELISA. Results: ADAMTS-4 IHC expression was significantly higher in interstitial compartment (INT) of NKB and TXCI group in peritubular capillaries (PTC) and interstitial stroma (INT). Patients with higher stages of interstitial fibrosis (ci > 1 and IFTA > 1) expressed ADAMTS-4 in INT more frequently in both groups (p = 0.005; p = 0.013; respectively). In paired comparison, TXCI samples expressed ADAMTS-4 in INT and PTC more often than TX0. ADAMTS-4 plasma concentration varied significantly across CKD stages, being highest in CKD 2 and 3 compared to other groups (p = 0.0064). Hemodialysis patients had higher concentrations of ADAMTS-4 compared to peritoneal dialysis (p < 0.00001). Conclusion: ADAMTS-4 might have a significant role in CKD as a potential novel diagnostic indicator.
Keywords: ADAMTS-4; bone morphogenic protein 1; chronic kidney disease; kidney transplantation; renal dialysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
