

Anchoring Apparatus of Long Head of the Biceps Tendon: Ultrasonographic Anatomy and Pathologic Conditions
- PMID: 35328211
- PMCID: PMC8947553
- DOI: 10.3390/diagnostics12030659
Anchoring Apparatus of Long Head of the Biceps Tendon: Ultrasonographic Anatomy and Pathologic Conditions
Abstract
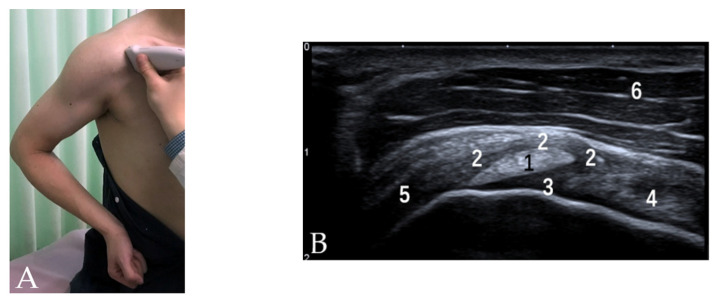
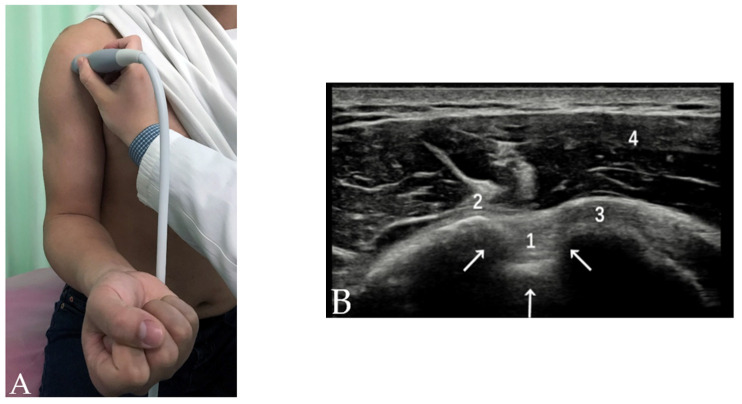
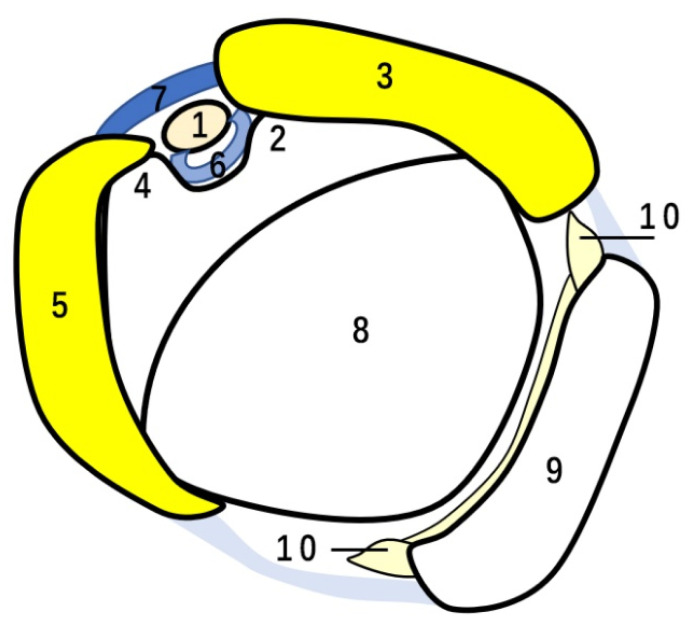
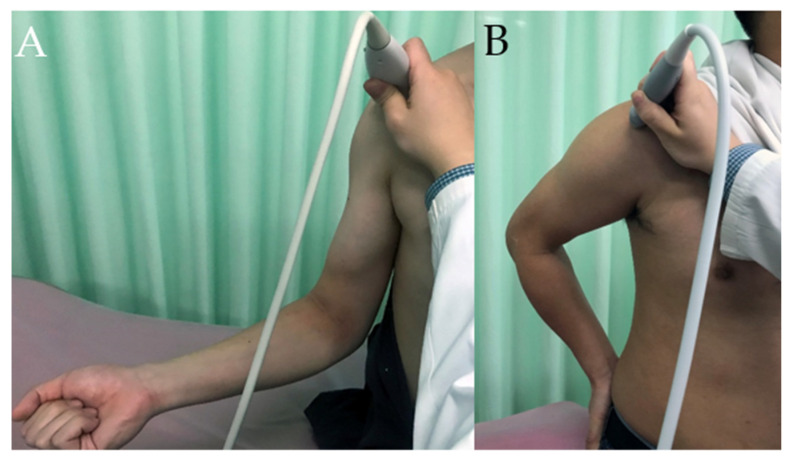
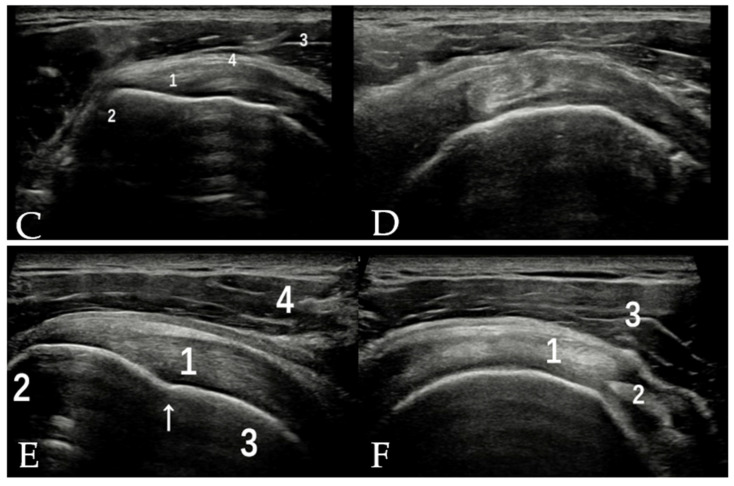
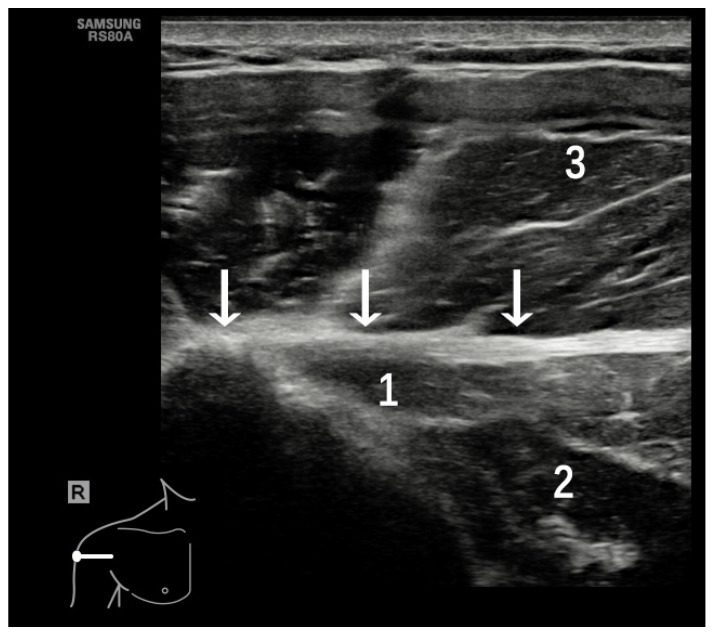
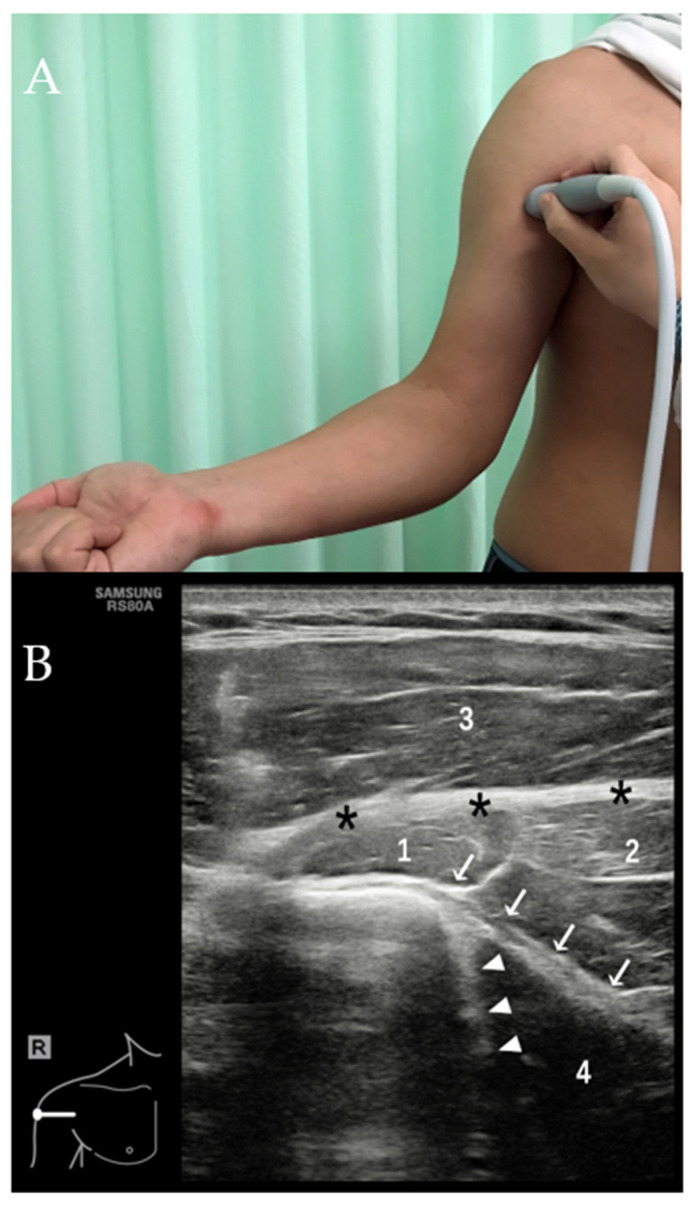
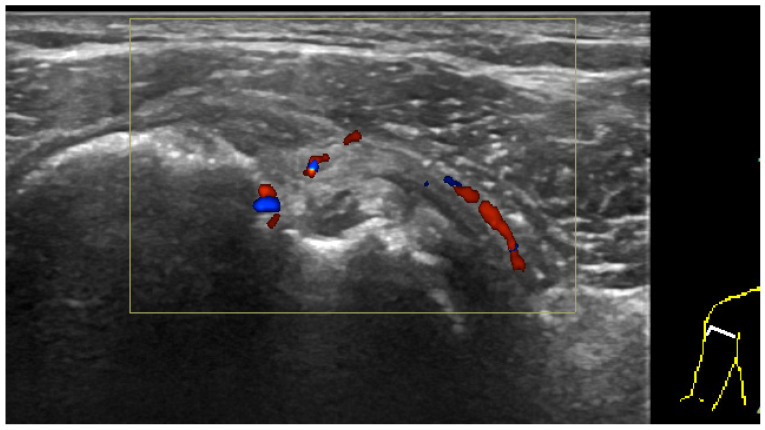
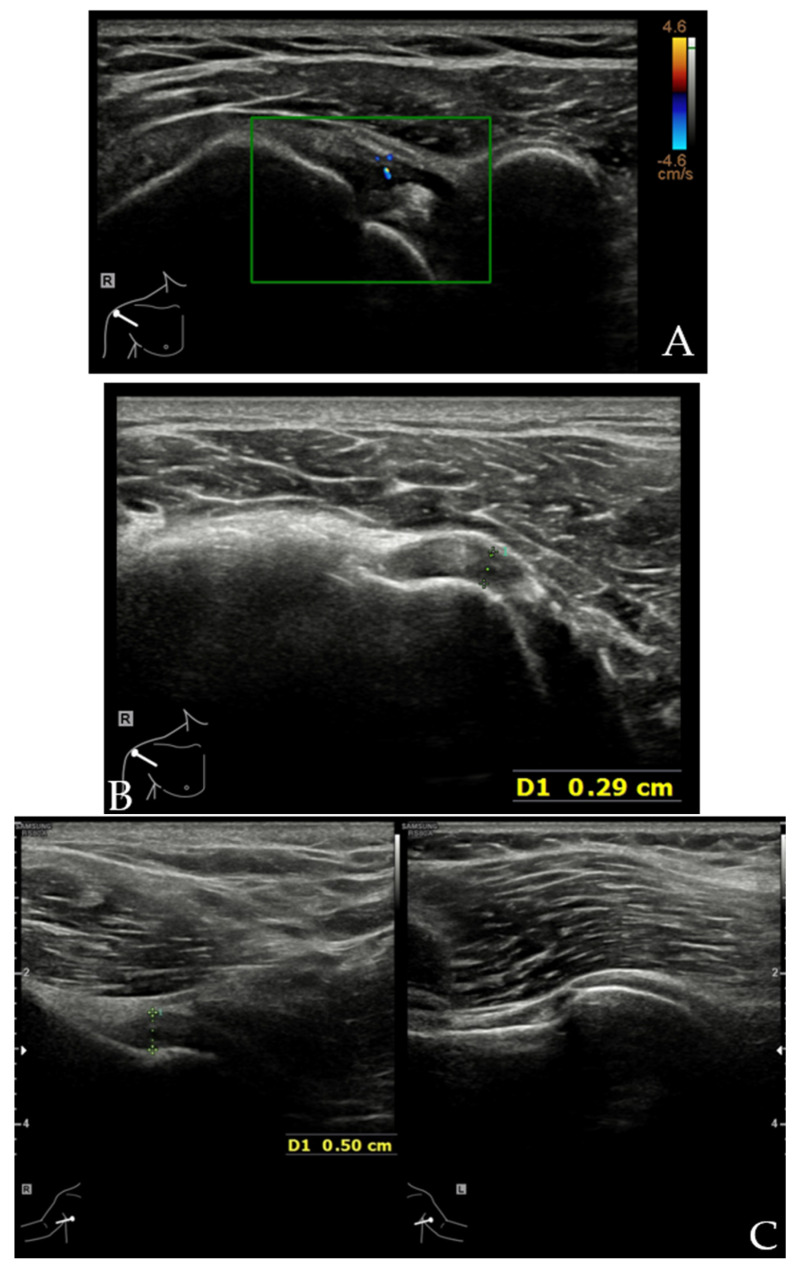
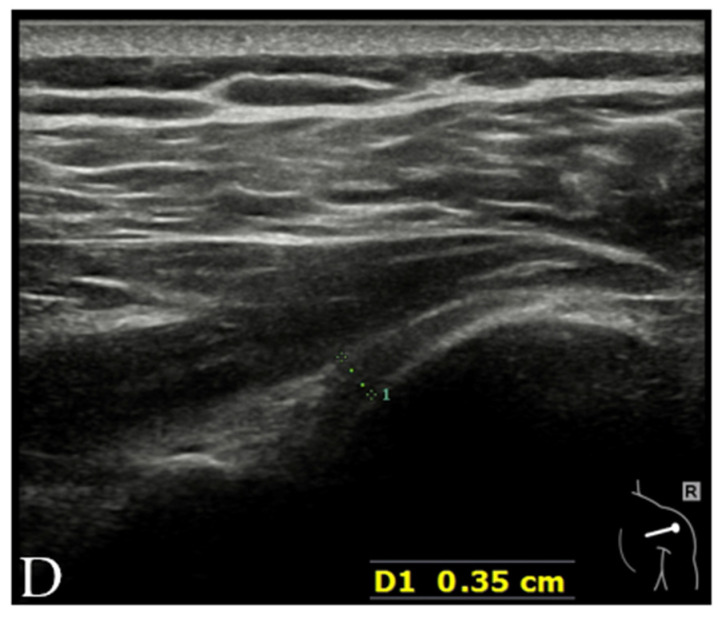
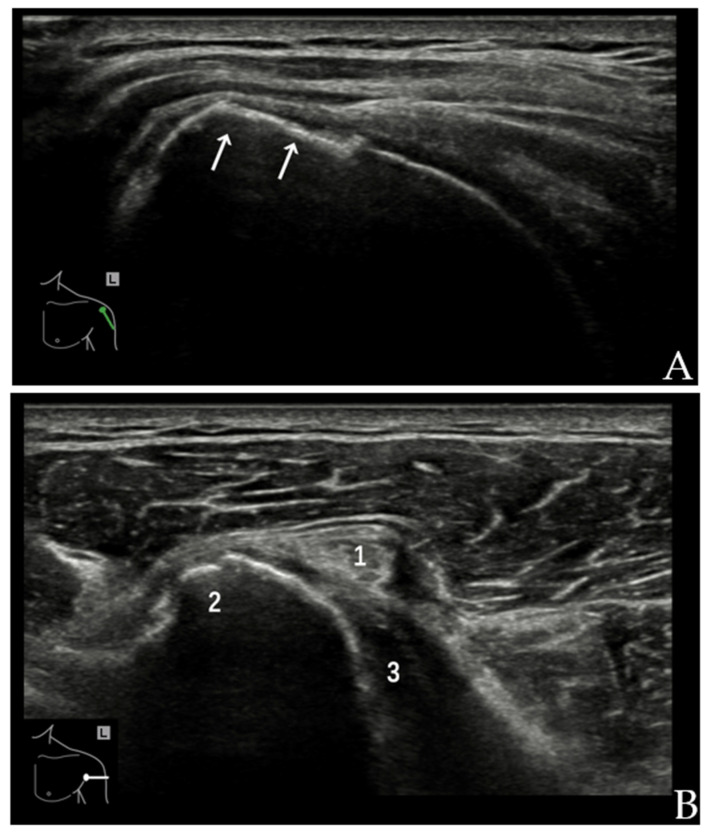
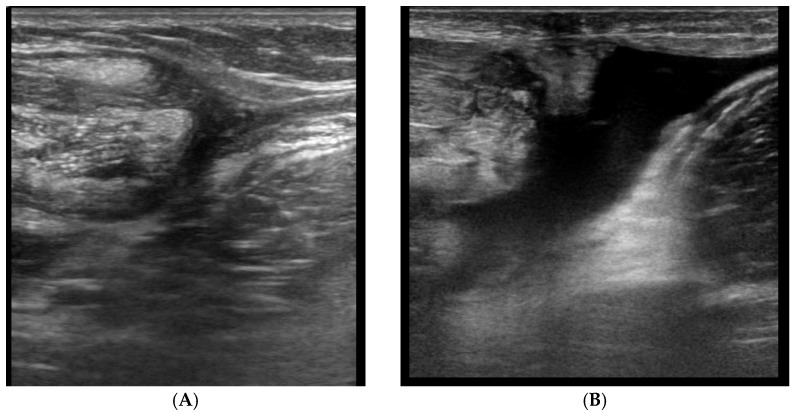
The long head of the biceps tendon (LHBT) has been recognized as an important generator of anterior shoulder pain, causing a significant reduction in the shoulder flexion range. Various tendinous and ligamentous structures form the anchoring apparatus of the LHBT along its course to maintain its appropriate location during shoulder movements, including the coracohumeral ligament (CHL), superior glenohumeral ligament (SGHL), subscapularis (SSC) tendon and supraspinatus (SSP) tendon as well as the less recognized tendons of pectoralis major (PM), latissimus dorsi (LD) and teres major (TM). Lesions of this stabilizing apparatus may lead to an instability of the LHBT, resulting in pain at the anterior shoulder. Ultrasonography (US) has been increasingly used in the assessment of shoulder injuries, including the anchoring apparatus of the LHBT. An accurate diagnosis of these injuries is often challenging, given the complex anatomy and wide spectrum of pathologies. In this review article, US anatomy and common pathologic conditions that affect the anchoring apparatus of the LHBT are discussed, including biceps pulley lesions, adhesive capsulitis, chronic pathology of SSC and SSP tendons, tears in the PM tendon and injuries to the LD and TM. Knowledge of a normal anatomy, an appropriate scanning technique and US findings of common pathologic conditions are the keys to accurate diagnoses.
Keywords: long head of the biceps tendon; rotator cuff; scanning technique; shoulder; ultrasonography.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Mellano C.R., Shin J.J., Yanke A.B., Verma N.N. Disorders of the long head of the biceps tendon. Instr Course Lect. 2015;64:567–576. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
